-
The Korean Antimicrobial Resistance Monitoring System for Complicated Urinary Tract Infections: A Prospective Multicenter Observational Study Conducted by the Korean Association of Urogenital Tract Infection and Inflammation
-
Seong Hyeon Yu, Seung Il Jung, Donghoon Lim, Jeong Woo Lee, Seung-Ju Lee, Hong Chung, Mi-Mi Oh, Jing Bong Choi, Jae Hung Jung, Hee Jo Yang, KAUTII Investigators
-
Urogenit Tract Infect 2026;21(1):15-25. Published online April 30, 2026
-
DOI: https://doi.org/10.14777/uti.2550040020
-
-
 Abstract Abstract
 PDF PDF PubReader PubReader
- Purpose
This study aimed to report antimicrobial resistance (AMR) patterns among patients with complicated urinary tract infection (cUTI) using data from the Korean Antimicrobial Resistance Monitoring System (KARMS).
Materials and Methods: In this prospective, multicenter, observational surveillance study, data from patients diagnosed with cUTI between January 2023 and September 2025 were retrieved from the KARMS database. Demographic characteristics, uropathogen distribution, and antimicrobial susceptibility profiles of representative pathogens were analyzed.
Results
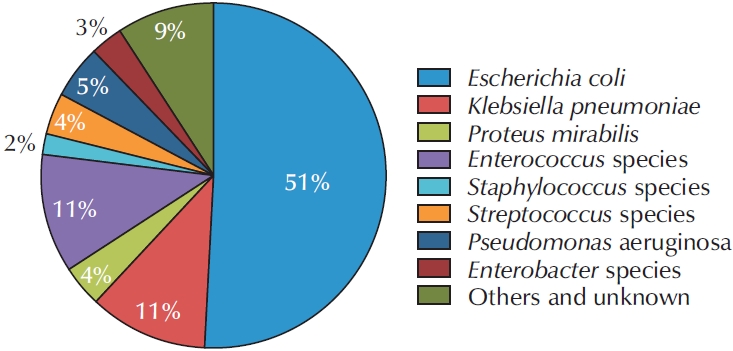
Data from a total of 698 patients were collected in the KARMS database. The mean patient age was 68.94±15.95 years. The numbers of patients with healthcare-associated UTI and recurrent UTI were 171 (24.5%) and 240 (34.4%), respectively. Escherichia coli was the most frequently identified uropathogen (n=356, 51.1%). Regarding antimicrobial susceptibility, 92.9% of isolates were susceptible to fosfomycin, 75.5% to nitrofurantoin, 47.2% to ciprofloxacin, 63.3% to cefotaxime, 80.6% to piperacillin/tazobactam, and 98.8% to ertapenem. The rate of extended-spectrum beta-lactamase positivity was 45.2% (166 of 367) and was significantly higher in pyelonephritis and urosepsis (62.3% and 62.5%, p=0.002), healthcare-associated UTI (58.6%, p=0.040), and recurrent cUTI (53.2%, p=0.028). Fluoroquinolone resistance was significantly more common in female patients (49.1%, p=0.021) and in healthcare-associated UTI (57.9%, p=0.014). Piperacillin/tazobactam resistance was significantly higher in patients with urosepsis (37.0%, p=0.004), in tertiary hospitals (17.2%, p=0.019), and in healthcare-associated UTI (26.4%, p=0.001). In addition, third-generation cephalosporin resistance was significantly higher in secondary hospitals than in tertiary hospitals (43.5% vs. 33.3%, p=0.041).
Conclusions
These data provide current information on uropathogen distribution and AMR patterns in cUTI in South Korea. Continued surveillance and ongoing data accumulation through KARMS will support evidence-based strategies for optimal antimicrobial therapy and AMR mitigation.
-
Korean Multicenter Study of Infectious Complications after Transurethral Prostate Surgery in Patients with Preoperative Sterile Urine
-
Seong Hyeon Yu, Seung Il Jung, Eu Chang Hwang, Tae-Hyoung Kim, Jae Duck Choi, Koo Han Yoo, Jeong Woo Lee, Dong Hoon Koh, Sangrak Bae, Seung Ok Yang, Joongwon Choi, Seung Ki Min, Hoon Choi
-
Urogenit Tract Infect 2022;17(3):81-88. Published online December 31, 2022
-
DOI: https://doi.org/10.14777/uti.2022.17.3.81
-
-
Abstract
PDFPubReader
 ePub ePub
- Purpose: To evaluate the efficacy of antibiotic prophylaxis and determine the risk factors of infectious complications after transurethral surgery of the prostate.
Materials and Methods: Seven hundred and seventy-two patients who underwent transurethral resection of the prostate (TURP) or holmium laser enucleation of the prostate (HOLEP) were reviewed. Of these, this study enrolled 643 patients without bacteriuria who had not received antibiotics for urinary tract infections for two weeks before surgery. The patients were divided into two groups according to the duration of the antibiotics (Group 1: less than one day, n=396 vs. Group 2: more than one day, n=247).
Results: The overall incidence of postoperative infectious complications in 643 patients was 5.0% (32/643). When postoperative infectious complications were compared according to the duration of the antibiotics (Group 1 vs. Group 2), the infectious complications rates were 5.6% (22/396) vs. 4.0% (10/247), respectively (p=0.393). When postoperative infectious complications were compared according to the duration of antibiotics (Group 1 vs. Group 2) in the TURP and HOLEP groups, the infectious complications rates were 6.3% (12/192) vs. 1.0% (1/103) (p=0.035) and 4.9% (10/203) vs. 6.0% (8/134) (p=0.677), respectively. The duration of Foley catheterization was independently associated with infectious complications (p=0.003).
Conclusions: The results showed that prolonged postoperative catheterization affects postoperative infectious complications associated with transurethral prostate surgery. Although antibiotics administered for less than one day are effective for antibiotic prophylaxis of transurethral prostate surgery, a longer antibiotic therapy is recommended for TURP.
-
Citations
Citations to this article as recorded by  - Evaluation of Postoperative Urinary Tract Infection and Sepsis Rates After Adding Cystolitholapaxy to HoLEP:
A Retrospective Analysis
Federico Rovegno, Rajiv Pillai, Zafar Maan, Soumendra Datta, Omar Nasir, Gerald Rix
International Journal of Clinical Urology.2026; 10(1): 1. CrossRef
-
4,931
View
-
35
Download
-
1
Crossref
-
Care of Voiding Dysfunction in Rehabilitation and Convalescent Hospitals
-
Seong Hyeon Yu, Eu Chang Hwang, Seung Il Jung
-
Urogenit Tract Infect 2021;16(2):32-43. Published online August 31, 2021
-
DOI: https://doi.org/10.14777/uti.2021.16.2.32
-
-
Abstract
PDFPubReaderePub
- The number of rehabilitation and convalescent hospitals is increasing rapidly; the primary goal of these institutions is to manage patients’ chronic disorders and maintain their daily functions. Most patients in these hospitals are elderly and experience difficulties related to behavior, communication, or cooperation because of various co-existing chronic medical diseases. Therefore, urologic problems may be more prevalent in these hospitals compared to other hospitals. On the other hand, unlike the medical management of other chronic medical problems, urologic problems have been neglected. This situation could increase the secondary complications, decrease the quality of life, and exacerbate co-existing conditions among such patients. Therefore, this review investigates problems concerning voiding dysfunction-related care in rehabilitation and convalescent hospitals and seeks solutions to overcome them.
-
Citations
Citations to this article as recorded by - The Korean Antimicrobial Resistance Monitoring System for Complicated Urinary Tract Infections: A Prospective Multicenter Observational Study Conducted by the Korean Association of Urogenital Tract Infection and Inflammation
Seong Hyeon Yu, Seung Il Jung, Donghoon Lim, Jeong Woo Lee, Seung-Ju Lee, Hong Chung, Mi-Mi Oh, Jing Bong Choi, Jae Hung Jung, Hee Jo Yang
Urogenital Tract Infection.2026; 21(1): 15. CrossRef
-
4,726
View
-
16
Download
-
1
Crossref
-
Optimal Modified Extended Antibiotic Prophylaxis for Prostate Biopsy: The Addition of Two Intravenous Doses of Amikacin to Ciprofloxacin
-
Seong Hyeon Yu, Seung Il Jung, Myung Soo Kim, Ho Seok Chung, Dong Deuk Kwon
-
Urogenit Tract Infect 2018;13(3):72-78. Published online December 31, 2018
-
DOI: https://doi.org/10.14777/uti.2018.13.3.72
-
-
Abstract
PDF
- Purpose: This retrospective study was undertaken to investigate whether increasing amikacin dosage for ciprofloxacin prophylaxis in patients with fluoroquinolone (FQ)-resistant rectal flora reduce infectious complications after transrectal ultrasound-guided prostate biopsy (TRUSPB).
Materials and Methods: A total of 430 patients with FQ-resistant rectal flora based on rectal swab cultures were divided into two groups. Patients in both groups were administered ciprofloxacin (400 mg, intravenous [IV], twice daily) on the same day as TRUSPB and one day after biopsy. However, whereas group 1 patients (n=202) were administered a single injection of amikacin (1g, IV) one hour before TRUSPB, patients in group 2 (n=228) were administered two injections of amikacin (1g, IV) before one hour TRUSPB and again on the day after TRUSPB.
Results: Of the 430 study subjects, 129 (30.0%) showed extended-spectrum beta-lactamase (ESBL) positivity. The overall incidence rate of infectious complications was 2.8% (12/430). Infectious complication rates were 4.0% (8/202) in group 1 and 1.3% (3/228) in group 2 (p=0.075). Urinary tract infection and acute prostatitis were more frequent in group 1 (3.5% vs. 0.4%, p=0.029). Infectious complication rates in ESBL negative patients were 3.4% (5/145) in group 1 and 1.3% (2/156) in group 2, whereas those in ESBL positive patients were 7.0% (4/57) in group 1 and 1.4% (1/72) in group 2.
Conclusions: Increasing the dosage of amikacin for ciprofloxacin prophylaxis reduce infectious complications in patients with FQ-resistant rectal flora and to be more effective in ESBL positive patients with FQ-resistant rectal flora.
-
Risk Factors of Infectious Complications after Transurethral Prostate Surgery in Patients with Preoperative Sterile Urine
-
Eu Chang Hwang, Seong Hyeon Yu, Jong Beom Kim, Seung Il Jung, Taek Won Kang, Dong Deuk Kwon, Kwangsung Park
-
Korean J Urogenit Tract Infect Inflamm 2013;8(1):27-31. Published online April 30, 2013
-
-
-
Abstract
PDF
- Purpose: To determine the risk factors of infectious complications after transurethral surgery of the prostate in patients with sterile urine.
Materials and Methods: A total of 183 patients who underwent transurethral resection of the prostate or holmium laser enucleation of the prostate were reviewed. All patients had urinalyses and urine cultures preoperatively, on the day of catheter removal, and at two weeks postoperatively. Patients were divided into two groups according to whether preoperative urinalysis showed sterile urine (group I, n=99) or not (group II, n=84). Clinical parameters were compared between the two groups. Univariate and multivariate logistic regression were used for estimation of infectious complications after surgery in group I.
Results: Compared with group II, group I showed younger age, fewer post voided residuals, low prostate specific antigen levels, short-term duration of oral antibiotic therapy, and low incidence of infectious complications (p<0.05). In univariate analysis in group I, age, diabetes mellitus (DM), prostate volume, resection weight, and duration of oral antibiotic therapy showed an association with infectious complications (p<0.05). Factors showing independent association with infectious complications in group I were DM (odds ratio [OR], 7.31; 95% confidence interval [CI], 1.83-29.0; p=0.005), resection weight (OR, 1.03; 95% CI, 1.01-1.06; p=0.039), and duration of oral antibiotics (OR, 0.64; 95% CI, 0.43-0.94; p=0.025).
Conclusions: Kinds of antibiotics showed no effect on infectious complication, therefore, second generation cephalosporin is recommended for reduction of antibiotic resistance. Clinicians should be aware of the high risk for infectious complication in patients with DM and who underwent large volume resection of the prostate.
|