


Articles
- Page Path
- HOME > Urogenit Tract Infect > Volume 16(2); 2021 > Article
- Review Care of Voiding Dysfunction in Rehabilitation and Convalescent Hospitals
-
Seong Hyeon Yu
 , Eu Chang Hwang, Seung Il Jung
, Eu Chang Hwang, Seung Il Jung -
Urogenital Tract Infection 2021;16(2):32-43.
DOI: https://doi.org/10.14777/uti.2021.16.2.32
Published online: August 31, 2021
Department of Urology, Chonnam National University Medical School, Gwangju, Korea
-
Correspondence to: Seung Il Jung,https://orcid.org/0000-0003-4864-8175' target='_blank'> , Department of Urology, Chonnam National University Hwasun Hospital, 322 Seoyang-ro, Hwasun-eup, Hwasun 58128, Korea, Tel: +82-61-379-7749, Fax: +82-61-379-7750, E-mail: drjsi51@gmail.com">drjsi51@gmail.com
• Received: August 11, 2021 • Revised: August 20, 2021 • Accepted: August 20, 2021
Copyright © 2021, Korean Association of Urogenital Tract Infection and Inflammation. All rights reserved.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 5,348 Views
- 16 Download
- 1 Crossref
Abstract
- The number of rehabilitation and convalescent hospitals is increasing rapidly; the primary goal of these institutions is to manage patients’ chronic disorders and maintain their daily functions. Most patients in these hospitals are elderly and experience difficulties related to behavior, communication, or cooperation because of various co-existing chronic medical diseases. Therefore, urologic problems may be more prevalent in these hospitals compared to other hospitals. On the other hand, unlike the medical management of other chronic medical problems, urologic problems have been neglected. This situation could increase the secondary complications, decrease the quality of life, and exacerbate co-existing conditions among such patients. Therefore, this review investigates problems concerning voiding dysfunction-related care in rehabilitation and convalescent hospitals and seeks solutions to overcome them.
INTRODUCTION
The term “rehabilitation and convalescent hospital” (RCH) refers to a medical institution that combines the functions of a hospital and a nursing institution. In general, such institutions guarantee long-term hospitalization. Rather than treating acute illness, their main aim is to help patients manage chronic disorders, maintain their conditions, and prevent a decrease in daily function. Recently, the number of RCHs and their medical costs have increased rapidly due to socio-environmental changes, including the rapidly aging population and the subsequent increase in chronic medical diseases. For example, the number of such hospitals has increased two-fold compared to their number 10 years ago (from 637 in 2008 to 1,582 in 2020), resulting in an estimated 5.5 billion dollars in health care costs [1] (Fig. 1).
Urologic problems, including incontinence or other voiding difficulties, are more common in RCHs than in other types of hospitals. These hospitals mostly treat elderly patients who tend to experience difficulties in behavior, communication, or cooperation. Furthermore, dementia, cerebral infarction, Parkinson’s disease, and spinal cord injuries are more prevalent in these hospitals. Moreover, these conditions are often accompanied by urologic problems [2,3]. Therefore, proper urologic problem management in RCHs is crucial for improving the quality of life (QoL), reducing secondary complications, encouraging early return to society, and decreasing the socioeconomic costs.
On the other hand, urologic problems have not been managed optimally for many reasons, including a lack of certified urologists and nursing staff who actually care about the urologic problems in RCHs, a paucity of standardized urologic assessment tools tailored to real-world practice, and the current health insurance systems in South Korea [1,4]. For these reasons, this review examined the problems related to voiding dysfunction care in RCHs to find solutions to overcome such problems.
BACKGROUND: VOIDING DYSFUNCTION IN ELDERLY
Aging inevitably brings certain structural and functional changes in various organ systems, including the genitourinary system. For example, bladder capacity may remain relatively stable or decrease slightly with aging [5,6]. Aging may also decrease the bladder wall’s smooth muscle-to-collagen ratio; this process is related to impaired bladder smooth muscle contraction and involuntary detrusor contractions [7,8]. Aging can also cause other structural changes, including alterations in the sensory receptors and neurotransmitters in the urothelium, which may, in turn, affect the bladder’s sensory and motor functions [9].
Aging-related anatomical changes in genitourinary systems can also affect lower urinary tract functions. In elderly women, pelvic organ prolapse associated with the body mass index, parity, or a history of pelvic surgery or radiotherapy can be linked to impaired voluntary voiding or stress urinary incontinence (UI) [9,10]. Moreover, benign prostatic hypertrophy (BPH) in elderly men may compress the urethra, causing an anatomic bladder outlet obstruction (BOO) [11].
Furthermore, aging-related changes in cognition and executive functions can affect the lower urinary tract symptoms (LUTS) dependent on (or independent of) specific changes to the lower urinary tract. Smith et al. [12] used functional imaging studies to suggest that brain abnormalities could increase the prevalence of urinary dysfunction, including overactive bladder and urge incontinence, in elderly individuals. Finally, polypharmacy is common in elderly individuals, and many non-urologic medications, including anti-dementia drugs, antipsychotics, antidepressants, bronchodilators, and opioids, could increase the anticholinergic burden and impairing the detrusor contractions [13,14]. Hashimoto et al. [14] reported that medications with an anticholinergic burden are commonly prescribed to people receiving LUTS treatment. Table 1 lists the contributing factors for voiding dysfunction in the elderly.
In summary, the abovementioned reasons can complicate the evaluation and management of elderly individuals with LUTS. Therefore, the role of the urologic specialist has become more emphasized compared to the past, particularly in RCHs with a high proportion of elderly patients.
THE PREVALENCE OF UROLOGIC DISEASES IN RCHS
As mentioned above, urologic problems tend to be more prevalent in RCHs because of many contributing conditions, including the high proportion of elderly patients, symptomatic and functional impairment, cognition, comorbidities, and polypharmacy. A 1981 US report showed that 69.3% of elderly patients in geriatric long-term care hospitals presented with urinary dysfunction; 38.3%, 20.2%, and 10.8% had incontinence, used a urinary diversion device, and were symptomatic without incontinence, respectively [15]. A population-based study by Suh et al. [16], who investigated the status of urologic diseases in South Korean geriatric hospitals from 2002 to 2013, reported a 24.5% prevalence of urologic disease in geriatric hospitals—2.1 times higher than the 11.5% found in general hospitals. Furthermore, their study showed that the diagnosis of all major voiding disorders was more frequent in geriatric hospitals. The relative risk for BPH, overactive bladder, and a neurogenic bladder was 1.9, 1.3, and 1.8, respectively [16].
Lee et al. [4] investigated the prevalence of urologic diseases in 13 South Korean geriatric hospitals. They reported that, among 1,858 patients, 48.4% had voiding difficulties, 50.1% had UI, and 64% had both conditions. Almost half of the incontinent patients (45.8%) suffered from severe incontinence (i.e., patients required at least five pads per day). Furthermore, 28.6% had at least one diagnosed urologic disorder, such as urinary tract infection (UTI), benign prostatic hyperplasia (BPH), or neurogenic bladder, at that time of admission. Regarding urologic complications, 20.2% had urologic complications related to voiding difficulty, including UTI, acute or chronic urinary obstruction, chronic renal failure, or urolithiasis, and 18.8% had secondary complications related to urologic diseases, including pressure sore or dermatitis. The total prevalence of urologic complications was 39.0%, including duplicates [4].
Incontinence is the most common urologic problem in RCHs. Its reported prevalence was 43-77% in US patients [17] and 42-50% in South Korean patients [4,18].
THE MANAGEMENT STATUS OF UROLOGIC DISEASES IN RCHS
Urologic problems occur frequently among elderly populations and are strongly associated with the QoL [19]. However, because most urologic diseases are not life-threatening, they have been neglected by health care providers [20]. Furthermore, in January 2008, the medical reimbursement system utilized in South Korean RCHs changed from a “fee-for-service” system to a “fixed sum medical fee per day” (FSMFD), which provides a fixed daily medical insurance fee. The new medical reimbursement system was graded based on the patient’s disease status, possible daily living activity, and required medical resources. The adoption of FSMFD began to affect the management of urologic problems adversely, and the trend of neglecting urologic disease worsened. To overcome this problem, FSMFD was revised in November 2019, and an adequacy assessment of RCH was introduced. On the other hand, the trend of neglecting urologic disease has continued.
Several investigators have reported the management status of urologic diseases in RCHs. Lawhorne et al. [20] reported that, in US nursing facilities, physicians were more likely to be involved in evaluating and managing behavioral symptoms, such as dementia, pain, falls, delirium, and unintended weight loss, than UI. In South Korea, Shin et al. [18] reported that most patients with incontinence were not managed immediately and that treatment was decided based on the cost and healthcare provider convenience. Their results showed that 74.8% were dependent on diapers all day, while only 7.5% managed their issues by taking urologic-related medications [18]. A later study by Lee et al. [4] reported that 20.7% were taking voiding disorder-related medications and 59.7% were managing their issues using a urinary intervention: diapers (53.3%), indwelling catheters (19.5%), clean intermittent catheters (CICs) (12.2%), or external collection urinary drainage (7.9%). On the other hand, only 7% were managed by a urologist, and 83% received no medical advice for their voiding problems [4].
Suh et al. [16] compared the prescription rates for urologic disease in RCHs and general hospitals. They reported pre-and post-FSMFD adoption changes and found that the prescription rate was 1.5 times higher in RCHs during the pre-FSMFD-adoption period. This figure dropped to only 0.3 times higher after that. Surprisingly, the propensity matching analysis for the same population of this study between two types of hospitals showed that the prescription rates of alpha-blockers, 5-alpha reductase inhibitors, anticholinergics, and antidiuretics were all lower in RCHs [16].
The lack of certified urologists in RCHs can also adversely affect the management of urologic diseases. According to the statistics from South Korea in December 2020 (Table 2), the number of urologists working in RCHs was 58, which is only 2.2% of the total number of urologists (2,610) and 1% of the total specialists working in RCHs. The number of urologists is significantly lower than those of other specialists in RCHs, such as obstetricians and gynecologists (6.2%, 372 of 5,906), and even pediatricians (2.6%, 156 of 5,840) [1]. This problem can result in the inaccurate diagnosis and treatment of urologic diseases, which, in turn, could complicate the immediate responses to urologic problems, thereby increasing patient mortality [21]. Lee et al. [4] reported that the diagnosis rate for urologic diseases in RCHs was less than 5%. Moreover, this diagnosis was always conducted by a non-urologist [4].
VARIOUS VOIDING DYSFUNCTIONS IN RCHS
Thus far, the management status and problems related to urologic diseases in RCHs have been identified. On the other hand, it is essential to know the various types of voiding dysfunctions in RCHs to overcome these issues.
UI, one of the most challenging geriatric syndromes, can affect approximately 30% of elderly people living in a given community, 50% of elderly residents in long-term care facilities, and 40% to 70% of hospitalized elderly people [22]. Many elderly patients in RCHs are vulnerable to UI because it is often associated with impairments in physical activity, mobility, balance, cognition, and nutrition [9]. Moreover, UI can lead to medical morbidity, decreased self-esteem, early institutionalization, increased caregiver stress, and considerable financial costs [23]. Therefore, UI management should be a significant concern for RCHs.
UI can be caused by various lower urinary tract conditions, including overactive bladder, underactive bladder, BOO, detrusor hyperactivity, and impaired contractility, as well as anatomical disorders, such as pelvic organ prolapse in women and post-radical prostatectomy status in men [9,13,24]. Therefore, because of the magnitude of its occurrence and consequences, UI-related treatment decisions are often complex and must be made with care, particularly in RCHs.
Among elderly patients with UI, behavioral interventions, including prompted voiding, toilet training, and time voiding, have often been considered conservative treatment mainstays. International consultation on incontinence has recommended combining toileting and exercise therapies that incorporate strengthening exercises and mobility skills with toileting routines [25]. In practice, this treatment has been applied to the FSMFD system in South Korean RCHs, and it is recommended in the treatment of elderly patients with UI. Unfortunately, it has not been implemented properly due to nursing staff shortages [1,4].
Several medical treatment options can be applied for UI management, including anticholinergic medication and β-3 agonist [13]. These drugs are mainly directed toward decreasing the detrusor hyperactivity. Therefore, they can be administered to patients with UI in RCHs. However, the post-void residual (PVR) should be measured before these drugs can be administered because a large amount of PVR could worsen the patientsʼ symptoms if they have other pre-existing voiding disorders, including BOO, detrusor underactivity, and neurogenic bladder conditions [9]. The International Continence Society consensus suggests that an ultrasound PVR of more than 50 ml after double voiding could indicate a suspicious voiding dysfunction [26]. On the other hand, the clinical impact of an elevated PVR remains controversial because PVR can increase gradually, and voiding volume decreases gradually with age [27]. Furthermore, anticholinergic medication has many side effects, including dry mouth, constipation, visual disturbances, gastroesophageal reflux disease, tachycardia, urinary retention, and certain side effects on the central nervous system, to which elderly patients may be particularly susceptible [13,23,28]. Given these considerations, clinicians should be careful while administering UI drugs and consulting urologists to ensure proper management wherever necessary.
Surgical interventions, including Onabotulinum toxinA [29], posterior tibial nerve stimulation [30], and sacral neuromodulation [31], can be considered for treating medication-refractory UI, even though the literature has rarely focused on the elderly population. Therefore, careful patient selection is necessary, and appropriate intervention by a urologist is mandatory.
The International Continence Society defines acute urinary retention (AUR) as a condition where “a patient cannot pass any urine despite having a full bladder, which on examination is painfully distended and readily palpable or percussible.” Furthermore, chronic urinary retention (CUR) is characterized as “a generally (but not always) painless and palpable or percussible bladder, where there is a chronic high PVR and where the patient experiences slow flow and incomplete bladder emptying” [26]. A 2016 American Urologic Association white paper on non- neurogenic chronic urinary retention defined CUR as “an elevated PVR of >300 ml that has persisted for at least six months and has been documented on two or more separate occasions.” [32] Contrary to CUR, AUR is commonly considered a painful occurrence and a common urologic emergency [33]. On the other hand, both conditions can be caused by increasing age, medications, BPH, LUTS, diabetes, cerebrovascular accident, neurological disorders, or postoperative settings [32-35]. Furthermore, because these conditions are more prevalent in RCHs, they are commonly encountered by all RCH-based health care providers, not just urologists.
When AUR and CUR are left untreated, they can lead to bladder rupture, gross hematuria, UTI, catheterization, hydronephrosis, and decreased renal function [33]. Furthermore, particularly in RCHs, the sequelae of AUR and CUR may be vicious because they can lead to decreased QoL, increased secondary complications, a delayed return to society, and additional medical costs. For example, a catheter-related urinary tract infection (CAUTI) that is traced to urinary retention can cause a significant degree of patient morbidity and medical cost in the US and the UK [36,37]. Previous systematic reviews have estimated these costs to include amounts anywhere from $876 (for the simplest attributable CAUTI costs of additional tests and therapies) to more than $10,000 (in payments for patients with significant complexity, e.g., intensive care unit patients with secondary bacteremia) [36].
Several possible medical interventions can prevent AUR. Avoiding medications that increase the chances of developing AUR (e.g., alpha-adrenergic agonists and anticholinergics) can reduce the incidence of AUR. Table 3 lists some common medications and their accompanying mechanisms that can contribute to AUR. Among patients with an indwelling foley catheter, delayed catheter removal [38] and the use of an alpha-blocker before catheter removal [39] are possible options for reducing AUR. Recently, Oelke et al. [40] reported that men treated with α-blockers, 5α-reductase inhibitors, or any combinations had lower AUR incidence rates than the general symptomatic population. Regarding CUR, the treatments for elderly patients should minimize pharmacological interventions that can contribute to urinary retention and maintain good bowel function and mobility. Retention-related disease statuses, such as neurological disorders and diabetes, should be managed properly. Furthermore, medical or surgical therapy should be applied to the effective management of underlying LUTS and for ensuring adequate bladder emptying. The American Urologic Association recommended frequent PVR use. They validated QoL questionnaires for supplementing routine laboratory studies, suggesting that these can be useful screening mechanisms for detecting worsening CUR [33].
The most common AUR treatment method is the placement of an indwelling Foley catheter. Furthermore, CIC has also been recommended for AUR treatments because the risk of CAUTI with short-term catheterization has been reported to increase up to 5% per day [34]. Suprapubic tube presents a preferable alternative option for urethral catheterization if the latter is impossible or if cystoscopic catheter placement cannot be performed [33]. As mentioned above, CIC can reduce symptomatic UTIs and subsequent urosepsis despite the weak evidence from related research literature and relatively high cost; therefore, CIC may be preferable to indwelling catheters for patients with CUR [41]. A minimum of four to six hours of CIC is recommended for minimizing the bacterial residence time [42]. On the other hand, CIC is used inadequately in RCHs. For example, Lee et al. [4] reported that only 12.2% of patients with urologic problems were treated with CIC. Moreover, their study of 13 South Korean geriatric hospitals showed that none of the patients were catheterized more than three times a day [4].
For urinary retention caused by BPH, bladder neck obstruction/contracture, or urethral stricture, minimal invasive surgical therapies, such as transurethral resection, laser procedures, and direct visual urethrotomy, should be initially considered [33,34,43].
Degenerative neurologic diseases are often accompanied by lower urinary tract dysfunction; it is one of the most common autonomic disorders with an estimated incidence of 27-80% [44]. The most common degenerative neurologic disease is Alzheimer’s disease, followed by Parkinson’s disease [44]. Several studies have reported that lower urinary tract health can significantly influence QoL, early institutionalization, and health economics [45,46]. Furthermore, LUTS have been associated with falling, which, in turn, can lead to increased mortality, particularly among patients with degenerative neurologic diseases in RCHs [47].
UI, one of the most common LUTS in patients with dementia, has a prevalence of 11-93% [23]. In particular, Ouslander et al. [48] reported that 65% of incontinent individuals had fewer than three incontinence episodes per week, 11% had three to six episodes per week, and 24% had one episode a day or more. McLaren et al. [49] reported that 90% of incontinent individuals had at least one incontinence episode during the three-week assessment period, 78% had one episode a week, and 40% had one episode a day. Urge UI is the most common type of UI in patients with Alzheimer’s disease [2]. Parkinson’s disease presents both storage symptoms (e.g., urgency, frequency, nocturia, and incontinence) and voiding symptoms (e.g., hesitancy, slow or interrupted stream, and double voiding), ranging from 38 to 71%. An overactive bladder is the most common LUTS in Parkinson’s disease [44,50].
The LUTS presented in degenerative neurologic disease can be caused by the disease itself [51], the neurological and urologic medication [52], and an aging bladder or other comorbidities. The LUTS onset and severity usually correlate with the disease progression and parallels with other autonomic dysfunctions [53,54]. UI, a common LUTS in patients with dementia, is frequently associated with decreasing motivation, cognitive disability, and gait disorder [23]. Therefore, conservative treatment (methods have been mentioned previously in this paper; please see the paragraph about incontinence) should be considered in the early stages of a disease’s trajectory. On the other hand, little evidence has supported specific behavioral strategies for patients with dementia [55-57].
Some neurological medical therapies can contribute to LUTS, such as acetylcholinesterase inhibitors (AChEIn) for treating dementia and levodopa or a dopamine agonist for treating Parkinson’s disease. AChEIn can affect cognition and memory function in the central nervous system and the peripheral urinary tract, particularly regarding bladder activity. Several studies have reported that AChEIn has an approximate risk of 7% risk for precipitating UI, and it is associated with significant worsening of UI [58,59]. Regarding levodopa and dopamine agonists, some studies have reported a worsening of bladder functions, even though they provide limited evidence for an association between these medications and impaired bladder function [60-62].
As mentioned in the previous paragraph, anticholinergic medication can be used for the first-line treatment of overactive bladder symptoms. On the other hand, current evidence suggests that anticholinergic medications, particularly oxybutynin, can lead to cognitive worsening because they can cross the blood–brain barrier and bind to the M1 receptors [23,63]. Among these, trospium does not cross a healthy blood–brain barrier [64]. Other studies have shown that solifenacin can pass the blood–brain barrier but becomes less bound to the M1 receptors [65], and propiverine can pass the blood–brain barrier to a minor extent [66]. Therefore, fewer central nervous system side effects can be expected. Of course, anticholinergic-induced cognitive impairment can be reversed through the discontinuation of relevant drugs [67]. Nevertheless, these pharmacokinetic mechanisms should be considered when prescribing such drugs to patients with degenerative neurological diseases. Furthermore, clinicians should prescribe anticholinergics more judiciously to patients already taking AChEIn because of the risk of exacerbating anticholinergic-induced central nervous system side effects. Recently, research has suggested mirabegron (β-3 agonist) as a potential treatment option for overactive bladder symptoms in elderly patients because it has the theoretical advantage of avoiding anticholinergic effects [68], but further studies will be needed necessary to verify the efficacy of the β-3 agonist.
In summary, the LUTS treatment in patients with degenerative neurologic disease should be customized to individual patientsʼ needs and disease statuses. Therefore, such treatments should consider factors, such as mobility, cognitive function, and general medical condition. Furthermore, given their special expertise, consultation or collaboration with a urologist should be considered, particularly in cognitively impaired and frail older patients in RCHs.
Spinal cord injury (SCI) is a prevalent condition. Approximately 12,000 to 17,000 new SCI s occur per year, according to the update series of the American Urologic Association [69]. Recent research has reported that this incidence rose dramatically in men aged 65 to 74 years because of the tendency of this demographic to suffer more traumatic falls [70]. In general, urinary frequency, urgency, and incontinence issues are common after an SCI [71]. These symptoms can indicate low bladder compliance, urinary calculi, bowel complications, and UTIs. Among these conditions, UTIs pose a significant problem for SCI patients because, if left untreated, they can lead to significant morbidity, including pyelonephritis or sepsis [72]. Conversely, SCI patients may receive over screening and treatment for suspected UTIs, which can lead to antibiotic resistance and increase their financial burden. Therefore, diagnosing, treating, and preventing UTIs in SCI patients is a complex and ongoing challenge.
A positive urine culture and concomitant symptoms are essential for diagnosing UTIs among SCI patients. Unlike the general population, which has UTI symptoms, such as urinary frequency, urgency, change in urine color or odor, and suprapubic pain, SCI patients present fewer typical UTI symptoms because of changes in their sensory functions. Consequently, other symptoms, including new-onset weakness, significantly increased spasticity or dysreflexia, increased UI, and confusion, are considered while diagnosing UTIs in SCI patients [69,73]. Routine urine culture is necessary for diagnosing UTIs in SCI patients because it can aid in correctly identifying bacteria and selecting proper antibiotics. Furthermore, when assessing UTIs for SCI patients who already have indwelling urinary catheters, urine culture should be obtained using a new urinary catheter and collection bag [69].
In general, SCI patients are particularly vulnerable to contracting UTIs within the first year of injury [74] and have the highest risk of contracting hospital-acquired UTIs during the initial hospitalization [75]. The most common bacteria associated with hospital-acquired infections in SCI patients is Escherichia coli, followed by Klebsiella, Enterococcus, and Enterobacter. Moreover, SCI patients frequently contract multidrug-resistant UTIs, leading to prolonged hospital stays [75]. In particular, SCI patients with positive proteus urine cultures may face increased hospitalization and morbidity risk because of decubitus ulcers and urinary stones [76].
In SCI patients, UTI-related treatments should only be performed for symptomatic, culture-proven UTIs. The Infectious Diseases Society of America recommended that no treatment be applied to asymptomatic bacteriuria in SCI patients. Exceptions should be made only in the case of patients undergoing invasive urologic procedures [77]. Although there is no consensus regarding the appropriate duration for antibiotics application, research has recommended that clinicians can choose a five- to seven-day antibiotics plan for SCI patients with new UTIs presenting without fevers, seven- to 10-day treatment for those with recurrent UTIs without fevers, and 14 days for SCI patients with fevers [69,78,79]. A narrower spectrum oral antibiotic, such as nitrofurantoin, fosfomycin, or trimethoprim, should be the first choice for treating UTIs in SCI patients. Furthermore, fluoroquinolones can be considered for treating prior resistance or rapidly progressing infections [78]. Intravenous or intramuscular antibiotics are the recommended treatment options for patients with a risk of sepsis who present with highly resistant organisms. A broad-spectrum intravenous beta-lactam is usually recommended for SCI patients with severe UTIs who require immediate intravenous antibiotics before the specific organism can be identified on cultures; it can be applied for 72 hours until the result of the specific organisms and resistance on cultures is obtained [80]. The first step for CAUTI in SCI patients is changing the catheter; this can help to reduce the antibiotics treatment durations [81].
Regarding prevention of recurrent UTIs, antibiotics prophylaxis is not recommended for treating SCI patients without UTIs, even among those who perform CIC or have a suprapubic tube. Instead, eliminating the risk factors for UTIs in SCI patients, such as bladder overdistention, lower bladder compliance, detrusor sphincter dyssynergia, urinary calculi, prolong indwelling catheters, and neurogenic bowel, is more effective for enhancing prevention. Table 4 details the American Urological Associationʼs recommended possible interventions for each situation.
Overall, proper diagnosis, management, and prevention of urinary symptoms in SCI patients can improve the patientʼs QoL and reduce the disease and financial burden. Contrary to expectations, many SCI patients cannot effectively access urologists [82], particularly in RCHs [4]. Therefore, urologists should be able to participate more actively in SCI patient care teams in RCHs, and an appropriate system must be established for supporting such participation.
FUTURE DIRECTIONS
Several suggestions can help to resolve the problems related to voiding dysfunction care in RCHs. First, the simplest and most effective solution is the use of sufficient urologists, which would ensure systemic voiding dysfunction and infection control care for elderly individuals in RCHs. Under circumstances where it may be challenging to employ sufficient urologists, regular RCH visits by available urologists may present a more realistic alternative. Second, the inclusion of standardized urologic assessment criteria in currently utilized adequacy assessment systems in RCH may supplement problem solving in current urologic care. For example, the Korean Urological Association Insurance Committee suggested adding queries related to the “proportion of patients with indwelling catheters” and the “rate of catheter-associated urinary tract infection”. Through this, a revised adequacy assessment system is expected to improve voiding dysfunction care in RCHs. On the other hand, more supplementation should be provided because it can cause hospital managers to underestimate the urologic problems. Finally, it is necessary to organize task forces that include expert urologists to support voiding dysfunction care in RCHs. For example, the Korean Urological Association Urination Management Committee recommended the establishment of “elderly urination management centers,” which could help to decrease the patients’ medical and economic burden by maintaining sufficient equipment and manpower for delivering appropriate first aid, treating urination-related problems within three to four hours of visiting, and facilitating a return to the RCHs. Nevertheless, this initiative is still in its early planning stage, and several hurdles might hinder its progress.
CONCLUSIONS
In conclusion, the problems regarding voiding dysfunction care in RCHs are too serious to ignore. Therefore, along with urologists, all health care providers working in these hospitals and related administrative government agencies must collaborate to overcome this problem.
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
S.H.Y. wrote the manuscript. S.H.Y. and E.C.H. participated in the study design and performed the statistical analysis. S.I.J. participated in the study design and coordination and helped to draft the manuscript. All authors read and approved the final manuscript.
NOTES
Fig. 1
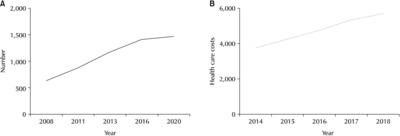
Number (A) and health care costs (B) in South Korean rehabilitation and convalescent hospitals. The costs are presented in KRW. 1 Unit: billion KRW.
Table 1
Contributing factors of voiding dysfunction in the elderly
Table 2
Number of specialists working in rehabilitation and convalescent hospitals
Table 3
Common medications and accompanying mechanisms that can contribute to acute urinary retention
Adapted from Acute and chronic urinary retention in men and women: epidemiology, treatment and future directions. Linthicum: American Urological Association; 2020. Available from: https://auau.auanet.org/content/update-series-volume-39-2020 [33].
Table 4
Risk factors for urinary tract infections in spinal cord injury patients and possible interventions
Adapted from Treatment and prevention of urinary tract infections in spinal cord injured patients. Linthicum: American Urological Association; 2020. Available from: https://auau.auanet.org/content/update-series-volume-39-2020 [69].
- 1. Healthcare Bigdata Hub. Health Insurance Statistics (Status of Hospital Institutions) [Internet]. Wonju: Health Insurance Review & Assessment Service; c2020 [cited 2021 Jul 10]. Available from: https://opendata.hira.or.kr/op/opc/selectHinsuStcInfo.do
- 2. Lee SH, Cho ST, Na HR, Ko SB, Park MH. Urinary incontinence in patients with Alzheimer's disease: relationship between symptom status and urodynamic diagnoses. Int J Urol 2014;21:683-7. PubMed
- 3. Jung HB, Kim HJ, Cho ST. A current perspective on geriatric lower urinary tract dysfunction. Korean J Urol 2015;56:266-75. ArticlePubMedPMC
- 4. Lee SH, Suh J, Kim HS, Lee YJ, Lee SR, Kim KH, et al. Prevalence and management status of urologic diseases in geriatric hospitals in South Korea: a field research. Investig Clin Urol 2017;58:70-6. ArticlePubMedPMCPDF
- 5. Pfisterer MH, Griffiths DJ, Schaefer W, Resnick NM. The effect of age on lower urinary tract function: a study in women. J Am Geriatr Soc 2006;54:405-12. ArticlePubMed
- 6. Pfisterer MH, Griffiths DJ, Rosenberg L, Schaefer W, Resnick NM. The impact of detrusor overactivity on bladder function in younger and older women. J Urol 2006;175:1777-83. discussion 1783. ArticlePubMed
- 7. Lowalekar SK, Cristofaro V, Radisavljevic ZM, Yalla SV, Sullivan MP. Loss of bladder smooth muscle caveolae in the aging bladder. Neurourol Urodyn 2012;31:586-92. ArticlePubMedPMCPDF
- 8. Elbadawi A, Yalla SV, Resnick NM. Structural basis of geriatric voiding dysfunction. II. Aging detrusor: normal versus impaired contractility. J Urol 1993;150(5 Pt 2):1657-67. ArticlePubMed
- 9. Hartigan SM, Reynolds WS, Smith PP. Dilemmas in management of the geriatric bladder. Curr Bladder Dysfunct Rep 2019;14:272-9. ArticlePubMedPMCPDF
- 10. Abrams P, Andersson KE, Birder L, Brubaker L, Cardozo L, Chapple C, et al. Members of Committees; Fourth International Consultation on Incontinence. Fourth International Consultation on Incontinence Recommendations of the International Scientific Committee: evaluation and treatment of urinary incontinence, pelvic organ prolapse, and fecal incontinence. Neurourol Urodyn 2010;29:213-40. PubMed
- 11. Patel ND, Parsons JK. Epidemiology and etiology of benign prostatic hyperplasia and bladder outlet obstruction. Indian J Urol 2014;30:170-6. ArticlePubMedPMC
- 12. Smith PP, Kuchel GA, Griffiths D. Functional brain imaging and the neural basis for voiding dysfunction in older adults. Clin Geriatr Med 2015;31:549-65. ArticlePubMed
- 13. Chung A, Noguchi N, Chan L, Tse V. Voiding dysfunction in older men. Curr Opin Urol 2016;26:177-83. ArticlePubMed
- 14. Hashimoto M, Hashimoto K, Ando F, Kimura Y, Nagase K, Arai K. Prescription rate of medications potentially contributing to lower urinary tract symptoms and detection of adverse reactions by prescription sequence symmetry analysis. J Pharm Health Care Sci 2015;1:7. ArticlePubMedPMCPDF
- 15. Jewett MA, Fernie GR, Holliday PJ, Pim ME. Urinarydysfunction in a geriatric long-term care population: prevalence and patterns. J Am Geriatr Soc 1981;29:211-4. ArticlePubMed
- 16. Suh J, Kim KH, Lee SH, Kim HS, Lee YJ, Lee SR, et al. Prevalence and management status of urologic disease in geriatric hospitals in South Korea: a population-based analysis. Investig Clin Urol 2017;58:281-8. ArticlePubMedPMCPDF
- 17. Offermans MP, Du Moulin MF, Hamers JP, Dassen T, Halfens RJ. Prevalence of urinary incontinence and associated risk factors in nursing home residents: a systematic review. Neurourol Urodyn 2009;28:288-94. ArticlePubMed
- 18. Shin CW, Kim SD, Cho WY. The prevalence and management of urinary incontinence in elderly patients at sanatorium in Busan area. Korean J Urol 2009;50:450-6. Article
- 19. Batista-Miranda JE, Molinuevo B, Pardo Y. Impact of lower urinary tract symptomson quality of life using Functional Assessment Cancer Therapy scale. Urology 2007;69:285-8. ArticlePubMed
- 20. Lawhorne LW, Ouslander JG, Parmelee PA, Resnick B, Calabrese B. Urinary incontinence: a neglected geriatric syndrome in nursing facilities. J Am Med Dir Assoc 2008;9:29-35. ArticlePubMed
- 21. Esparcia A, Artero A, Eiros JM, Balaguer M, Madrazo M, Alberola J, et al. Influence of inadequate antimicrobial therapy on prognosis in elderly patients with severe urinary tract infections. Eur J Intern Med 2014;25:523-7. ArticlePubMed
- 22. Melo LS, Ercole FF, Oliveira DU, Pinto TS, Victoriano MA, Alcoforado CLGC. Urinary tract infection: a cohort of older people with urinary incontinence. Rev Bras Enferm 2017;70:838-44. ArticlePubMed
- 23. Averbeck MA, Altaweel W, Manu-Marin A, Madersbacher H. Management of LUTS in patients with dementia and associated disorders. Neurourol Urodyn 2017;36:245-52. ArticlePubMedPDF
- 24. Griffiths DJ, McCracken PN, Harrison GM, Gormley EA, Moore KN. Urge incontinence and impaired detrusor contractility in the elderly. Neurourol Urodyn 2002;21:126-31. ArticlePubMed
- 25. Gibson W, Johnson T, Kirschner-Hermanns R, Kuchel G, Markland A, Orme S, et al. Incontinence in frail elderly persons: report of the 6th International Consultation on Incontinence. Neurourol Urodyn 2021;40:38-54. ArticlePubMedPDF
- 26. D'Ancona C, Haylen B, Oelke M, Abranches-Monteiro L, Arnold E, Goldman H, et al. Standardisation Steering Committee ICS and the ICS Working Group on Terminology for Male Lower Urinary Tract & Pelvic Floor Symptoms and Dysfunction. The International Continence Society (ICS) report on the terminology for adult male lower urinary tract and pelvic floor symptoms and dysfunction. Neurourol Urodyn 2019;38:433-77. ArticlePubMedPDF
- 27. Rule AD, Jacobson DJ, McGree ME, Girman CJ, Lieber MM, Jacobsen SJ. Longitudinal changes in post-void residual and voided volume among community dwelling men. J Urol 2005;174(4 Pt 1):1317-21. discussion 1321-2. author reply 1322. ArticlePubMed
- 28. Griebling TL. Overactive bladder in elderly men: epidemiology, evaluation, clinical effects, and management. Curr Urol Rep 2013;14:418-25. ArticlePubMedPDF
- 29. Jambusaria LH, Dmochowski RR. Intradetrusor onabotulinum-toxinA for overactive bladder. Expert Opin Biol Ther 2014;14:721-7. ArticlePubMed
- 30. Pratt TS, Suskind AM. Management of overactive bladder in older women. Curr Urol Rep 2018;19:92. ArticlePubMedPMCPDF
- 31. Faris AER, Gill BC, Pizarro-Berdichevsky J, Dielubanza E, Clifton MM, Okafor H, et al. Impact of age and comorbidities on use of sacral neuromodulation. J Urol 2017;198:161-6. ArticlePubMed
- 32. Stoffel J, Lightner D, Peterson A, Sandhu J, Suskind A, Wei J. Non-neurogenic chronic urinary retention: consensus definition, management strategies, and future opportunities [Internet]. Linthicum: American Urological Association; c2016 [cited 2021 Jul 11]. Available from: https://www.auanet.org/guidelines/guidelines/chronic-urinary-retention
- 33. Giblin BM, Kowalik U, Plante MK. Acute and chronic urinary retention in men and women: epidemiology, treatment and future directions [Internet]. Linthicum: American Urological Association; c2020 [cited 2021 Jul 11]. Available from: https://auau.auanet.org/content/update-series-volume-39-2020
- 34. Kowalik U, Plante MK. Urinary retention in surgical patients. Surg Clin North Am 2016;96:453-67. ArticlePubMed
- 35. Özveren B, Keskin S. Presentation and prognosis of female acute urinary retention: analysis of an unusual clinical condition in outpatients. Urol Ann 2016;8:444-8. ArticlePubMedPMC
- 36. Hollenbeak CS, Schilling AL. The attributable cost of catheter-associated urinary tract infections inthe United States: a systematic review. Am J Infect Control 2018;46:751-7. ArticlePubMed
- 37. Smith DRM, Pouwels KB, Hopkins S, Naylor NR, Smieszek T, Robotham JV. Epidemiology and health-economic burden of urinary-catheter-associated infection in English NHS hospitals: a probabilisticmodelling study. J Hosp Infect 2019;103:44-54. ArticlePubMed
- 38. Lee SY, Kang SB, Kim DW, Oh HK, Ihn MH. Risk factors and preventive measures for acute urinary retention after rectal cancer surgery. World J Surg 2015;39:275-82. ArticlePubMedPDF
- 39. Zeif HJ, Subramonian K. Alpha blockers prior to removal of a catheter for acute urinary retention in adult men. Cochrane Database Syst Rev 2009;4:CD006744. Article
- 40. Oelke M, Speakman MJ, Desgrandchamps F, Mamoulakis C. Acute urinary retention rates in the general male population and in adult men with lower urinary tract symptoms participating in pharmacotherapy trials: a literature review. Urology 2015;86:654-65. ArticlePubMed
- 41. Kidd EA, Stewart F, Kassis NC, Hom E, Omar MI. Urethral (indwelling or intermittent) or suprapubic routes for short-term catheterisation in hospitalised adults. Cochrane Database Syst Rev 2015;12:CD004203. Article
- 42. Wyndaele JJ, Brauner A, Geerlings SE, Bela K, Peter T, Bjerklund-Johanson TE. Clean intermittent catheterization and urinary tract infection: review and guide for future research. BJU Int 2012;110(11 Pt C):E910-7. ArticlePubMed
- 43. Raison N, Challacombe B. Opening the flood gates: holmium laser enucleation is superior to photoselective vaporization of the prostate for the treatment of chronic urinary retention. BJU Int 2015;115:178-9. ArticlePubMed
- 44. Sakakibara R, Panicker J, Finazzi-Agro E, Iacovelli V, Bruschini H. Parkinson's Disease Subcomittee, The Neurourology Promotion Committee in The International Continence Society. A guideline for the management of bladder dysfunction in Parkinson's disease and other gait disorders. Neurourol Urodyn 2016;35:551-63. ArticlePubMed
- 45. McGrother CW, Jagger C, Clarke M, Castleden CM. Handicaps associated with incontinence: implications for management. J Epidemiol Community Health 1990;44:246-8. ArticlePubMedPMC
- 46. Sakakibara R, Shinotoh H, Uchiyama T, Sakuma M, Kashiwado M, Yoshiyama M, et al. Questionnaire-based assessment of pelvic organ dysfunction in Parkinson's disease. Auton Neurosci 2001;92:76-85. ArticlePubMed
- 47. Bower WF, Whishaw DM, Khan F. Nocturia as a marker of poor health: causal associations to inform care. Neurourol Urodyn 2017;36:697-705. ArticlePubMedPDF
- 48. Ouslander JG, Zarit SH, Orr NK, Muira SA. Incontinence among elderly community-dwelling dementia patients. Characteristics, management, and impact on caregivers. J Am Geriatr Soc 1990;38:440-5. PubMed
- 49. McLaren SM, McPherson FM, Sinclair F, Ballinger BR. Prevalence and severity of incontinence among hospitalized, female psychogeriatric patients. Health Bull (Edinb) 1981;39:157-61. PubMed
- 50. Sakakibara R, Tateno F, Kishi M, Tsuyuzaki Y, Uchiyama T, Yamamoto T. Pathophysiology of bladder dysfunction in Parkinson's disease. Neurobiol Dis 2012;46:565-71. ArticlePubMed
- 51. Toba K, Ouchi Y, Orimo H, Iimura O, Sasaki H, Nakamura Y, et al. Urinary incontinence in elderly inpatients in Japan: a comparison between general and geriatric hospitals. Aging (Milano) 1996;8:47-54. ArticlePubMedPDF
- 52. Campbell AJ, Reinken J, McCosh L. Incontinence in the elderly: prevalence and prognosis. Age Ageing 1985;14:65-70. ArticlePubMed
- 53. Leung KS, Ng MF, Pang FC, Au SY. Urinary incontinence: an ignored problem in elderly patients. Hong Kong Med J 1997;3:27-33. PubMed
- 54. Magerkurth C, Schnitzer R, Braune S. Symptoms of autonomic failure in Parkinson's disease: prevalence and impact on daily life. Clin Auton Res 2005;15:76-82. ArticlePubMedPDF
- 55. Jirovec MM, Templin T. Predicting success using individualized scheduled toileting for memory-impaired elders at home. Res Nurs Health 2001;24:1-8. ArticlePubMed
- 56. Engberg S, Sereika SM, McDowell BJ, Weber E, Brodak I. Effectiveness of prompted voiding in treating urinary incontinence in cognitively impaired homebound older adults. J Wound Ostomy Continence Nurs 2002;29:252-65. ArticlePubMed
- 57. Drennan VM, Greenwood N, Cole L, Fader M, Grant R, Rait G, et al. Conservative interventions for incontinence in people with dementia or cognitive impairment, living at home: a systematic review. BMC Geriatr 2012;12:77. ArticlePubMedPMCPDF
- 58. Starr JM. Cholinesterase inhibitor treatment and urinary incontinence in Alzheimer's disease. J Am Geriatr Soc 2007;55:800-1. ArticlePubMed
- 59. Gill SS, Mamdani M, Naglie G, Streiner DL, Bronskill SE, Kopp A, et al. A prescribing cascade involving cholinesterase inhibitors and anticholinergic drugs. Arch Intern Med 2005;165:808-13. ArticlePubMed
- 60. Uchiyama T, Sakakibara R, Hattori T, Yamanishi T. Short-term effect of a single levodopa dose on micturition disturbance in Parkinson's disease patients with the wearing-off phenomenon. Mov Disord 2003;18:573-8. ArticlePubMed
- 61. Berger Y, Blaivas JG, DeLaRocha ER, Salinas JM. Urodynamic findings in Parkinson's disease. J Urol 1987;138:836-8. ArticlePubMed
- 62. Sugiyama T, Hashimoto K, Kiwamoto H, Ohnishi N, Esa A, Park YC, et al. Urinary incontinence in senile dementia of the Alzheimer type (SDAT). Int J Urol 1994;1:337-40. ArticlePubMed
- 63. Kay G, Crook T, Rekeda L, Lima R, Ebinger U, Arguinzoniz M, et al. Differential effects of the antimuscarinic agents darifenacin and oxybutynin ER on memory in older subjects. Eur Urol 2006;50:317-26. ArticlePubMed
- 64. Staskin D, Kay G, Tannenbaum C, Goldman HB, Bhashi K, Ling J, et al. Trospium chloride has no effect on memory testing and is assay undetectable in the central nervous system of older patients with overactive bladder. Int J Clin Pract 2010;64:1294-300. ArticlePubMed
- 65. Sakakibara R, Panicker J, Fowler CJ, Tateno F, Kishi M, Tsuyusaki Y, et al. Is overactive bladder a brain disease? The pathophysiological role of cerebral white matter in the elderly. Int J Urol 2014;21:33-8. Article
- 66. Sakakibara R, Ogata T, Uchiyama T, Kishi M, Ogawa E, Isaka S, et al. How to manage overactive bladder in elderly individuals with dementia? A combined use of donepezil, a central acetylcholinesterase inhibitor, and propiverine, a peripheral muscarine receptor antagonist. J Am Geriatr Soc 2009;57:1515-7. ArticlePubMed
- 67. Gray SL, Anderson ML, Dublin S, Hanlon JT, Hubbard R, Walker R, et al. Cumulative use of strong anticholinergics and incident dementia: a prospective cohort study. JAMA Intern Med 2015;175:401-7. ArticlePubMedPMC
- 68. Krauwinkel W, van Dijk J, Schaddelee M, Eltink C, Meijer J, Strabach G, et al. Pharmacokinetic properties of mirabegron, a β3-adrenoceptor agonist: results from two phase I, randomized, multiple-dose studies in healthy young and elderly men and women. Clin Ther 2012;34:2144-60. ArticlePubMed
- 69. Stoffel JT. Treatment and prevention of urinary tract infections in spinal cord injured patients [Internet]. Linthicum: American Urological Association; 2020 [cited 2021 Jul 11]. Available from: https://auau.auanet.org/content/update-series-volume-39-2020
- 70. Jain NB, Ayers GD, Peterson EN, Harris MB, Morse L, O'Connor KC, et al. Traumatic spinal cord injury in the United States, 1993-2012. JAMA 2015;313:2236-43. ArticlePubMedPMC
- 71. Myers JB, Lenherr SM, Stoffel JT, Elliott SP, Presson AP, Zhang C, et al. Patient reported bladder related symptoms and quality of life after spinal cord injury with different bladder management strategies. J Urol 2019;202:574-84. ArticlePubMed
- 72. Welk B, Liu K, Winick-Ng J, Shariff SZ. Urinary tract infections, urologic surgery, and renal dysfunction in a contemporary cohort of traumatic spinal cord injured patients. Neurourol Urodyn 2017;36:640-7. ArticlePubMedPDF
- 73. Goetz LL, Cardenas DD, Kennelly M, Bonne Lee BS, Linsenmeyer T, Moser C, et al. International Spinal Cord Injury Urinary Tract Infection Basic Data Set. Spinal Cord 2013;51:700-4. ArticlePubMedPDF
- 74. Stillman MD, Barber J, Burns S, Williams S, Hoffman JM. Complications of spinal cord injury over the first year after discharge from inpatient rehabilitation. Arch Phys Med Rehabil 2017;98:1800-5. ArticlePubMed
- 75. Goodes LM, King GK, Rea A, Murray K, Boan P, Watts A, et al. Early urinary tract infection after spinal cord injury: a retrospective inpatient cohort study. Spinal Cord 2020;58:25-34. ArticlePubMedPDF
- 76. Hung EW, Darouiche RO, Trautner BW. Proteus bacteriuria is associated with significant morbidity in spinal cord injury. Spinal Cord 2007;45:616-20. ArticlePubMedPDF
- 77. Nicolle LE. Updated guidelines for screening for asymptomatic bacteriuria. JAMA 2019;322:1152-4. ArticlePubMed
- 78. Everaert K, Lumen N, Kerckhaert W, Willaert P, van Driel M. Urinary tract infections in spinal cord injury: prevention and treatment guidelines. Acta Clin Belg 2009;64:335-40. ArticlePubMed
- 79. Pannek J, Wöllner J. Management of urinary tract infections in patients with neurogenic bladder: challenges and solutions. Res Rep Urol 2017;9:121-7. ArticlePubMedPMCPDF
- 80. Dinh A, Davido B, Duran C, Bouchand F, Gaillard JL, Even A, et al. Urinary tract infections in patients with neurogenic bladder. Med Mal Infect 2019;49:495-504. ArticlePubMed
- 81. Darouiche RO, Al Mohajer M, Siddiq DM, Minard CG. Short versus long course of antibiotics for catheter-associated urinary tract infections in patients with spinal cord injury: a randomized controlled noninferiority trial. Arch Phys Med Rehabil 2014;95:290-6. ArticlePubMed
- 82. Cameron AP, Lai J, Saigal CS, Clemens JQ. NIDDK Urological Diseases in America Project. Urological surveillance and medical complications after spinal cord injury in the United States. Urology 2015;86:506-10. ArticlePubMed
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- The Korean Antimicrobial Resistance Monitoring System for Complicated Urinary Tract Infections: A Prospective Multicenter Observational Study Conducted by the Korean Association of Urogenital Tract Infection and Inflammation
Seong Hyeon Yu, Seung Il Jung, Donghoon Lim, Jeong Woo Lee, Seung-Ju Lee, Hong Chung, Mi-Mi Oh, Jing Bong Choi, Jae Hung Jung, Hee Jo Yang
Urogenital Tract Infection.2026; 21(1): 15. CrossRef
 ePub Link
ePub Link Cite
CiteCare of Voiding Dysfunction in Rehabilitation and Convalescent Hospitals
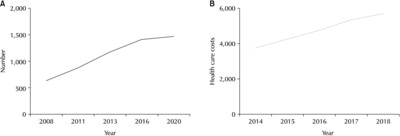
Fig. 1
Number (A) and health care costs (B) in South Korean rehabilitation and convalescent hospitals. The costs are presented in KRW. 1 Unit: billion KRW.
Fig. 1
Care of Voiding Dysfunction in Rehabilitation and Convalescent Hospitals
Contributing factors of voiding dysfunction in the elderly
| Structural and functional changes |
| Stable or decreasing bladder capacity |
| Decreasing smooth muscle of the bladder wall |
| Alterations in the sensory receptors and neurotransmitters in the urothelium |
| Anatomical changes |
| Pelvic organ prolapse |
| Benign prostatic hypertrophy |
| Pelvic surgery |
| Cognitive and executive function changes |
| Dementia |
| Parkinsonʼs disease |
| Cerebral infarction |
| Multiple system atrophy |
| Polypharmacy |
Number of specialists working in rehabilitation and convalescent hospitals
| Department | Total (n) | Rehabilitation and convalescent hospitals (n) | Proportion of specialists working in rehabilitation and convalescent hospitals (%) |
|---|---|---|---|
| Internal medicine | 16,921 | 864 | 5.10 |
| Neurology | 1,953 | 269 | 13.77 |
| Psychiatry | 3,794 | 546 | 14.39 |
| General surgery | 6,275 | 720 | 11.47 |
| Orthopedics | 6,574 | 213 | 3.24 |
| Neurosurgery | 2,913 | 206 | 7.07 |
| Chest surgery | 1,140 | 69 | 6.05 |
| Plastic surgery | 2,126 | 21 | 0.99 |
| Anesthesia | 4,888 | 98 | 2.00 |
| Obstetrics and gynecology | 5,906 | 372 | 6.30 |
| Pediatrics | 5,840 | 156 | 2.67 |
| Ophthalmology | 3,510 | 14 | 0.40 |
| Otorhinolaryngology | 3,977 | 41 | 1.03 |
| Dermatology | 2,290 | 8 | 0.35 |
| Urology | 2,610 | 58 | 2.22 |
| Radiology | 3,910 | 17 | 0.43 |
| Radiation oncology | 321 | 6 | 1.87 |
| Pathology | 885 | 9 | 1.01 |
| Laboratory medicine | 907 | 8 | 0.88 |
| Tuberculosis medicine | 57 | 5 | 8.77 |
| Rehabilitation medicine | 2,235 | 610 | 27.30 |
| Nuclear medicine | 247 | 2 | 0.81 |
| Family medicine | 6,935 | 1,071 | 15.44 |
| Emergency medicine | 1,913 | 20 | 1.05 |
| Occupational and environmental medicine | 560 | 2 | 0.36 |
| Preventive medicine | 190 | 4 | 2.11 |
These statistics were investigated in December 2020.
Common medications and accompanying mechanisms that can contribute to acute urinary retention
| Category | Mechanism |
|---|---|
| Alpha-adrenergic agonists | Increase urinary sphincter tone |
| Opioid pain medicines | Decrease bladder contractility |
| Nonsteroidal anti-inflammatory drugs | Decrease contractility through downregulation of prostaglandins |
| Calcium channel blockers, beta-adrenergic agonists | Decrease detrusor tone |
| Antidepressants, antipsychotics, antihistamines | Other |
Adapted from Acute and chronic urinary retention in men and women: epidemiology, treatment and future directions. Linthicum: American Urological Association; 2020. Available from:
Risk factors for urinary tract infections in spinal cord injury patients and possible interventions
| Risk factor | Possible interventions |
|---|---|
| Bladder overdistension | - Void or catheterize to keep volumes <400 ml |
| - Avoid obstruction of indwelling catheter | |
| Low bladder compliance | - Anticholinergic or beta-3 agonist medication |
| - Onabotulinum toxin injections | |
| - Bladder augment/urinary diversion | |
| Detrusor sphincter dyssynergia | - Reduce contractility of the bladder with anticholinergic medications or onabotulinum toxin |
| - Avoid spontaneous or reflexive voiding | |
| Urinary calculi | - Treat all bladder stones |
| - Treat all obstructing calculi | |
| - Treat renal calculi if staghorn | |
| Urinary catheterization | - Consider changing indwelling catheters to clean intermittent catheters |
| - Consider hydrophilic catheter when performing clean intermittent catheters | |
| Neurogenic bowel | - Promote regular bowel program |
Adapted from Treatment and prevention of urinary tract infections in spinal cord injured patients. Linthicum: American Urological Association; 2020. Available from:
Table 1
Contributing factors of voiding dysfunction in the elderly
Table 2
Number of specialists working in rehabilitation and convalescent hospitals
These statistics were investigated in December 2020.
Table 3
Common medications and accompanying mechanisms that can contribute to acute urinary retention
Adapted from Acute and chronic urinary retention in men and women: epidemiology, treatment and future directions. Linthicum: American Urological Association; 2020. Available from:
Table 4
Risk factors for urinary tract infections in spinal cord injury patients and possible interventions
Adapted from Treatment and prevention of urinary tract infections in spinal cord injured patients. Linthicum: American Urological Association; 2020. Available from:

