


Articles
- Page Path
- HOME > Urogenit Tract Infect > Volume 19(1); 2024 > Article
- Original Article Does Music Have a Calming Effect on Pain and Anxiety in Patients Undergoing Cystoscopy?
-
Ye Chan Joo1
 , Ji Eun Yu1, Jae Hyun Baik1, Young Seop Chang1, Jin Bum Kim1, Hyung Joon Kim1, Dong Hoon Koh1, Hong Wook Kim1,2
, Ji Eun Yu1, Jae Hyun Baik1, Young Seop Chang1, Jin Bum Kim1, Hyung Joon Kim1, Dong Hoon Koh1, Hong Wook Kim1,2 -
Urogenital Tract Infection 2024;19(1):3-9.
DOI: https://doi.org/10.14777/uti.2024.19.1.3
Published online: April 30, 2024
1Department of Urology, Konyang University Hospital, Konyang University College of Medicine, Daejeon, Korea
2Konyang University Myunggok Medical Research Institute, Daejeon, Korea
-
Correspondence to: Hong Wook Kim,https://orcid.org/0000-0002-3847-1401' target='_blank'> , Department of Urology, Konyang University Hospital, Konyang University College of Medicine, 24-19 Gwanjeobuk-ro 51beon-gil, Seo-gu, Daejeon 35360, Korea, Tel: +82-42-600-9480, Fax: +82-42-541-2879, E-mail: urokim@kyuh.ac.kr">urokim@kyuh.ac.kr
• Received: October 25, 2023 • Revised: April 17, 2024 • Accepted: April 17, 2024
Copyright © 2024, Korean Association of Urogenital Tract Infection and Inflammation. All rights reserved.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,761 Views
- 44 Download
Abstract
-
Purpose Cystoscopy is a diagnostic test performed frequently in urology outpatient clinics. Despite the large number of inspections, the associated pain, discomfort, or anxiety can markedly affect patient compliance and adherence to subsequent surveillance protocols. This study conducted a prospective, randomized study to investigate the potential efficacy of music and pyuria on pain or anxiety during outpatient cystoscopy.
-
Materials and Methods In this single-institution, randomized study, the participants were assigned to a music-intervention or non-music control group. The music-intervention group underwent an identical procedure with the addition of Johann Sebastian Bach’s “Air on the G String” from Suite No. 3 in D major, BWV 1068. Urinalysis was performed to determine if pyuria affects pain during the procedure.
-
Results The patient-reported outcomes, encompassing the changes in the STAI-X-1 (State-Trait Anxiety Inventory-X-1) scores, subjective levels of discomfort, embarrassment, satisfaction, and pain, were similar in the two groups. In contrast, the surgeons reported statistically significant differences in their evaluations of the same items as patient-reported outcomes of the two groups. The patient-reported pain showed no significant differences between the pyuria-negative group (0-2 and 3-5 WBC/HPF) and pyuria-positive group (>5 WBC/HPF).
-
Conclusions The data from this study do not support the hypothesis that musical intervention during cystoscopy alleviates pain or anxiety to any significant extent. In addition, pyuria did not affect the patient’s reported pain. Nevertheless, a notable impact was observed in the surgeons’ assessments, suggesting that the musical accompaniment may alter the surgeons’ perception of patient pain and anxiety levels throughout the procedure.
INTRODUCTION
Cystoscopy is one of the most frequently executed diagnostic and surveillance interventions in urological outpatient departments. According to 2022 statistics in Korea, approximately 173,000 cystoscopy procedures were undertaken, indicating an increasing use of this technique [1]. Despite being commonly practiced, the procedure may cause significant patient discomfort, manifesting as pain, and lower urinary tract symptoms such as frequency, urgency, and suprapubic pain, which in turn may compromise patient compliance in subsequent clinical interactions. In addition, the procedure can also cause urinary tract infections (UTIs), which can often be a source of pain [2,3]. Multiple modalities have been used to ameliorate such discomfort, including the systemic administration of analgesics and the instillation of lidocaine gel into the urethral canal or prophylactic antibiotics [4,5].
Among various mitigative approaches, musical inter-vention has been proposed to alleviate procedure-related discomfort and pain [6-8]. An extensive body of literature substantiates the efficacy of auditory stimulation in attenuating pain across various clinical contexts. Numerous studies delineate its positive effects in chronic pain management and diverse procedures, such as colonoscopy and colposcopy [9-14]. Moreover, music is a safe, cost-effective, and efficacious intervention in urological outpatient settings, devoid of adverse effects such as the addictive potential often associated with opioid analgesics [15]. On the other hand, McClintock et al. [16] failed to corroborate the hypothesis that music exerts analgesic or anxiolytic effects.
In light of these contrasting findings, this study assessed the potential role of music in alleviating pain and anxiety during outpatient cystoscopy. In addition, this study searched the relationship between the patient-reported pain and the presence of pyuria. Other physiological parameters, such as blood pressure and heart rate, were examined as part of a comprehensive assessment.
MATERIALS AND METHODS
A prospective, randomized, controlled trial was conducted at a single institution. This study received ethical approval from the Institutional Review Board of Konyang University Hospital (IRB No. 2023-05-053). Informed consent was obtained from each participant while they awaited the procedure. This study adhered to all ethical guidelines outlined in the 1964 Declaration of Helsinki and its subsequent amendments.
The subjects of this study were patients undergoing elective outpatient cystoscopy in the Department of Urology. The inclusion criteria were participants at least 19 years of age and of any gender. The exclusion criteria encompassed individuals with anatomical abnormalities in the urethra, those scheduled for procedures that could exacerbate pain, and individuals with auditory impairments that would preclude them from auditory interventions such as music.
The trial was powered to detect a difference of one point on a 10-point visual analog scale (VAS) for pain (converted to 10 points on a 100 mm VAS scale) and 10 points on the State-Trait Anxiety Inventory-X-1 (STAI-X-1). These predeter-mined metrics met or were below the minimally clinically significant differences defined in existing pain literature [17-19]. Based on these calculations, a sample size of 94 was determined to be sufficient for achieving statistical significance (47 in each group; p<0.05, power 0.90).
One hundred patients were recruited and randomized through coin-tossing to undergo the procedure with or without musical accompaniment. Five patients were excluded: two due to auditory impairments and three due to sound dilation before cystoscopy. Consequently, 50 patients were subjected to musical intervention during cystoscopy, while 45 served as the controls and underwent the procedure without music. Auditory intervention commenced immediately upon patient positioning and was delivered via a sound system adjacent to the procedural table.
Pre-procedurally, the patients’ perineal regions were prepared with betadine and received an intraurethral instillation of lidocaine gel. Subsequently, a flexible 16Fr and a rigid 17Fr cystoscope were used for male and female patients, respectively. Systemic analgesics were admi-nistered to some patients, either alone or in conjunction with lidocaine gel; a subset received neither. Musical accompaniment, when applied, consisted of the classical composition “Air on the G String” from Suite No. 3 in D major, BWV 1068. All procedures were performed by five clinicians adhering to a standardized protocol.
The patient’s anxiety levels were assessed pre- and post-procedure using the STAI-X-1, a self-report questionnaire consisting of 20 items scored on a four-point scale, with an overall score range of 20-80. The delta-STAI-X-1, representing the change in STAI-X-1 scores before and after the procedure, was calculated. A 100 mm VAS was used to evaluate post-procedural pain, discomfort, embarrassment, and satisfaction. The terminological ambiguity was mitigated by explaining the difference between ‘pain’ and ‘discomfort’ to patients based on standard definitions [20]. Surgeons were also requested to assess these parameters using identical questionnaires. The vital signs, namely heart rate and blood pressure, were monitored both pre- and post-procedure, serving as auxiliary indicators of the pain and anxiety levels.
A urinalysis prior to the procedure was performed by collecting the midstream urine sample to determine the presence of pyuria before the procedure and if pyuria affected pain during the procedure. The definition of pyuria was defined as the presence of more than five leukocytes/HPF in the urine [2].
The primary outcome of interest was the alleviation of pain. The secondary outcomes included differentiating other parameters, such as the vital signs and patient-reported discomfort.
Descriptive statistics were used, with parameters expressed as mean±, standard deviation, and range. Statistical analyses were conducted using SPSS Statistics version 26.0 (IBM Co.). Comparative assessments of the variables were conducted using the Student’s t-test for the continuous variables and a chi-square test for categorical variables. A p-value<0.05 was considered significant.
RESULTS
Ninety-five patients were incorporated into the study: 50 in the music group and 45 in the non-music group. Table 1 lists the demographic characteristics and procedural specifics. The average age of participants was 65.07 years, ranging from 29 to 92 years. The mean frequency of prior cystoscopies was distributed comparably between the two groups. Flexible cystoscopes were deployed in 69 cases, and rigid cystoscopes were utilized in 26 cases. The average pre-procedural waiting duration was 28 minutes, ranging from seven to 90 minutes, and showing no significant variations between the two groups.
Although the music group exhibited marginally superior mean values across parameters such as perceived procedure duration, discomfort, embarrassment, satisfaction, and pain, no statistically significant differences were found in these post-procedure patient-reported outcomes. Table 2 provi-des a comprehensive summary of these variables.
Every metric assessed from the post-procedure surgeons’ perspectives yielded statistically significant disparities. In particular, the actual procedure duration, quantified as 2.96±1.92 minutes, was considerably shorter than the duration perceived by patients, averaging 8.52±6.16 minutes. Furthermore, the surgeons reported improved VAS scores in terms of discomfort, embarrassment, satisfaction, and pain when juxtaposed with the patient-reported scores. Table 3 lists the results.
Table 4 lists the periprocedural data involving STAI-X-1 scores, Delta STAI-X-1 scores, and vital signs. No statistically significant differences in the measured parameters were observed between the two groups. There was no statistically significant difference between the two groups concerning the use of painkillers (p=0.348) (Supplement 1).
The patients were divided into two groups based on the presence or absence of pyuria (pyuria-positive group [n=30] and pyuria-negative group [n=65]) to determine if there was a difference in the pain scores between the groups; no significant difference was observed between two groups (p=0.071) (Fig. 1).
Subgroup analysis was performed according to previous cystoscopy experience, and the cystoscopy time was signi-ficantly longer in the group without a previous cystoscopy (3.12±2.43 vs. 2.77±0.99, p=0.016). Significant differences were noted in patient embarrassment (41.25±32.7 vs. 22.79±22.3, p=0.002) and the embarrassment of the surgeon (33.46±21.4 vs. 25.35±14.7, p=0.022) in the no previous cystoscopy group. Among the male group, only the patient procedure time (8.64±3.39 vs. 9.19±7.35, p=0.024) and patient satisfaction (75.24±21.75 vs. 67.88±30.0, p=0.027) were significantly different in the music and non-music groups. Among the female group, only the patient procedure time (2.38±0.74 vs. 3.78±2.69, p=0.035) was significantly different.
DISCUSSION
The summary of the study’s findings revealed two key points:
(1) The act of listening to classical music failed to produce any statistically significant reduction in either pain or anxiety levels in patients compared to the control group. This outcome was corroborated by the questionnaires filled out by the patients and the data gleaned from monitoring the vital signs.
(2) Interestingly, surgeons assessed the patient outcomes more favorably than the patients themselves, especially in terms of pain, discomfort, and other subjective experiences.
These results do not provide conclusive evidence that music has a soothing effect on pain and anxiety for patients undergoing outpatient cystoscopy.
This study exists within the broader context of a significant body of research probing the efficacy of music as a complementary or alternative approach to traditional methods, such as analgesics or sedation. Previous research often showed promising results for the capacity of music to relieve pain and anxiety in urological procedures like cystoscopy [10,12,21-23].
Despite these findings, this study did not show statistical significance, suggesting a discordance between prior studies and the present results [6-8]. This discrepancy is crucial because patients who experience post-procedure pain or discomfort may be less compliant with future necessary medical procedures, a concern that also negatively impacts the surgeons’ willingness to recommend cystoscopies [20].
Regarding the theoretical underpinning of why music might mitigate pain and anxiety, the explanation is likely multifactorial. Music engages cognitive activities that could potentially ameliorate the perceived intensity and unplea-sant-ness of pain [24]. Moreover, it has been speculated that music can activate certain neurotransmitters like dopamine, potentially influencing physiological systems such as the cardiovascular system [25].
The study was designed to be a prospective, randomized trial that minimizes the influence of confounding variables. It also used various measurement methods, from vital signs to various scales and questionnaires, to assess the patients’ and practitioners’ perspectives. Nevertheless, the study is not without limitations. Among them are the heterogeneity in painkiller use, anatomical differences between male and female subjects, too much variation in the VAS range that the patients reported, and inconsistencies in cystoscopy techniques among multiple surgeons. Furthermore, the study only used one type of classical music, limiting the generalizability of its findings to other musical compositions that might be more effective in reducing pain or anxiety [20].
In general, the guidelines recommend that tests be performed without inflammation, such as bacteriuria, before cystoscopy, but because this study included cystoscopies performed to check for hematuria, recurrent UTIs, and other causes, some tests were performed with positive pyuria. Therefore, the presence of pyuria did not make a statistically significant difference in the outcome of the study.
Future studies should address these limitations, possibly by standardizing the type of music used and the cystoscopy techniques and controlling for gender-specific anatomical differences that might affect the outcomes.
CONCLUSIONS
The current study showed no statistically significant benefits of using music to reduce pain or anxiety among patients undergoing cystoscopy, and pyuria was not a statistically significant factor that affected the pati-ent-reported pain. On the other hand, the surgeons’ assessments showed a notable difference, suggesting that music may have affected their perceptions of patient discomfort and anxiety during the procedure.
SUPPLEMENTARY MATERIALS
Supplementary data can be found via https://doi.org/10.14777/uti.2024.19.1.3.
ACKNOWLEDGMENTS
The authors thank the patients, nurses, and doctors who participated in this study.
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
FUNDING
This work was supported by Konyang University Myunggok Research Fund of 2014-07.
-
AUTHOR CONTRIBUTIONS
H.W.K. and H.J.K. participated in conceptualization. Y.C.J. and J.H.B. participated in data curation. Y.C.J. and J.E.Y. participated in formal analysis. H.W.K. and H.J.K. participated in methodology. Y.S.C., J.B.K., and D.H.K. participated in project administration. Y.C.J. participated in visualization and writing - original draft. H.W.K., H.J.K., and D.H.K. participated in writing - review & editing.
NOTES
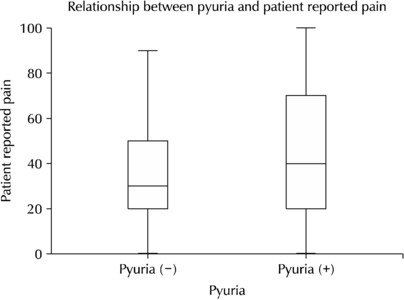
Table 1
Patient characteristics and procedure details
Table 2
Assessments by the patients following the intervention
Table 3
Post-procedure patient assessments by the surgeon
Table 4
Summary of the periprocedural anxiety parameter and vital signs
- 1. HIRA Bigdata Open portal. HIRA Bigdata Open portal [Internet]. Wonju: Health Insurance Review & Assessment Service (HIRA); c2023 [cited 2023 Jul 14]. Available from: https://opendata.hira.or.kr/op/opc/olapDiagBhvInfoTab1.do
- 2. Kim A, Ahn J, Choi WS, Park HK, Kim S, Paick SH, et al. What is the cause of recurrent urinary tract infection? Contemporary microscopic concepts of pathophysiology. Int Neurourol J 2021;25:192-201. ArticlePubMedPMCPDF
- 3. Khasriya R, Barcella W, De Iorio M, Swamy S, Gill K, Kupelian A, et al. Lower urinary tract symptoms that predict microscopic pyuria. Int Urogynecol J 2018;29:1019-28. ArticlePubMedPMCPDF
- 4. Stein M, Lubetkin D, Taub HC, Skinner WK, Haberman J, Kreutzer ER. The effects of intraurethral lidocaine anesthetic and patient anxiety on pain perception during cystoscopy. J Urol 1994;151:1518-21. ArticlePubMed
- 5. Jimenez-Pacheco A, Lardelli Claret P, Lopez Luque A, Lahoz-Garcia C, Arrabal Polo MA, Nogueras Ocana M. Randomized clinical trial on antimicrobial prophylaxis for flexible urethrocystoscopy. Arch Esp Urol 2012;65:542-9.PubMed
- 6. Yeo JK, Cho DY, Oh MM, Park SS, Park MG. Listening to music during cystoscopy decreases anxiety, pain, and dissatisfaction in patients: a pilot randomized controlled trial. J Endourol 2013;27:459-62. ArticlePubMedPMC
- 7. Gauba A, Ramachandra MN, Saraogi M, Geraghty R, Hameed BMZ, Abumarzouk O, et al. Music reduces patient-reported pain and anxiety and should be routinely offered during flexible cystoscopy: outcomes of a systematic review. Arab J Urol 2021;19:480-7. ArticlePubMedPMC
- 8. Chen G, Tang C, Liu Y, Liu Y, Dai Y, Yang L. Does listening to music improve pain perception and anxiety in patients undergoing cystoscopy: a meta-analysis. Front Surg 2021;8:689782. ArticlePubMedPMC
- 9. Garza-Villarreal EA, Pando V, Vuust P, Parsons C. Music-indu-ced analgesia in chronic pain conditions: a systematic review and meta-analysis. Pain Physician 2017;20:597-610. ArticlePubMed
- 10. Celebi D, Yilmaz E, Sahin ST, Baydur H. The effect of music therapy during colonoscopy on pain, anxiety and patient comfort: a randomized controlled trial. Complement Ther Clin Pract 2020;38:101084. ArticlePubMed
- 11. Jo JK, Kim YT. The diagnosis of chronic pelvic pain: how can we detect urological pain? Int Neurourol J 2022;26:87-91. ArticlePubMedPMCPDF
- 12. Abdelhakim AM, Samy A, Abbas AM. Effect of music in reducing patient anxiety during colposcopy: a systematic review and meta-analysis of randomized controlled trials. J Gynecol Obstet Hum Reprod 2019;48:855-61. ArticlePubMed
- 13. Culha Y, Ak ES, Culha MG. The effect of running water sound listened to patients during urodynamics on anxiety and urodynamic parameters. Int Neurourol J 2023;27:217-23. PubMedPMC
- 14. Jang EB, Hong SH, Kim KS, Park SY, Kim YT, Yoon YE, et al. Catheter-related bladder discomfort: how can we manage it? Int Neurourol J 2020;24:324-31. ArticlePubMedPMCPDF
- 15. Kyriakides R, Jones P, Geraghty R, Skolarikos A, Liatsikos E, Traxer O, et al. Effect of music on outpatient urological procedures: a systematic review and meta-analysis from the European Association of Urology Section of Uro-Technology. J Urol 2018;199:1319-27. ArticlePubMed
- 16. McClintock G, Wong E, Mancuso P, Lalak N, Gassner P, Haghighi K, et al. Music during flexible cystoscopy for pain and anxiety - a patient-blinded randomised control trial. BJU Int 2021;128 Suppl 1:27-32. ArticlePubMedPDF
- 17. Olsen MF, Bjerre E, Hansen MD, Hilden J, Landler NE, Tendal B, et al. Pain relief that matters to patients: systematic review of empirical studies assessing the minimum clinically important difference in acute pain. BMC Med 2017;15:35. ArticlePubMedPMCPDF
- 18. Corsaletti BF, Proenca MDGL, Bisca GKW, Leite JC, Bellinetti LM, Pitta F. Minimal important difference for anxiety and depression surveys after intervention to increase daily physical activity in smokers. Fisioter Pesqui 2014;21:359-64.
- 19. Suh J, Oh SJ, Cho SY. Comprehensive review of effective application of questionnaires for clinical research on lower urinary tract symptoms with translation and cultural adaptation to the Korean language. Int Neurourol J 2020;24:313-23. ArticlePubMedPMCPDF
- 20. Mumm JN, Eismann L, Rodler S, Vilsmaier T, Zehni AZ, Apfelbeck M, et al. Listening to music during outpatient cystoscopy reduces pain and anxiety and increases satis-faction: results from a prospective randomized study. Urol Int 2021;105:792-8. ArticlePubMedPDF
- 21. Lee DW, Chan KW, Poon CM, Ko CW, Chan KH, Sin KS, et al. Relaxation music decreases the dose of patient-controlled sedation during colonoscopy: a prospective randomized controlled trial. Gastrointest Endosc 2002;55:33-6. ArticlePubMed
- 22. Kulkarni S, Johnson PC, Kettles S, Kasthuri RS. Music during interventional radiological procedures, effect on sedation, pain and anxiety: a randomised controlled trial. Br J Radiol 2012;85:1059-63. ArticlePubMedPMCPDF
- 23. Gokcek E, Kaydu A. The effects of music therapy in patients undergoing septorhinoplasty surgery under general anes-thesia. Braz J Otorhinolaryngol 2020;86:419-26. ArticlePubMedPMC
- 24. Melzack R, Casey KL. In: Kenshalo DR, editor. Sensory, motivational, and central control determinants of pain: a new conceptual model. The skin senses. Charles C Thomas; 1968. p. 423-39.
- 25. Darki C, Riley J, Dadabhoy DP, Darki A, Garetto J. The effect of classical music on heart rate, blood pressure, and mood. Cureus 2022;14:e27348. ArticlePubMedPMC
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteDoes Music Have a Calming Effect on Pain and Anxiety in Patients Undergoing Cystoscopy?
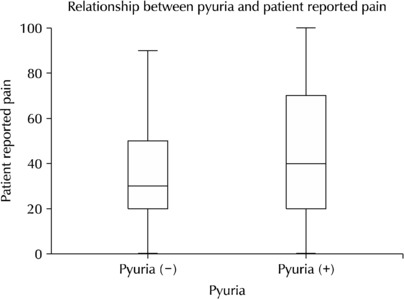
Fig. 1
Relationship between pyuria and patient-reported pain.
Fig. 1
Does Music Have a Calming Effect on Pain and Anxiety in Patients Undergoing Cystoscopy?
Patient characteristics and procedure details
| Characteristics | Music, n=50 | No music, n=45 | Total | p-value |
|---|---|---|---|---|
| Age (y) | 0.971 | |||
| Mean±SD | 65.12±13.91 | 65.02±12.12 | 65.07±13.03 | |
| Range | 33-92 | 29-83 | 29-92 | |
| Sex | 0.011 | |||
| Male | 42 (44.2) | 27 (28.4) | 69 (72.6) | |
| Female | 8 (8.4) | 18 (18.9) | 26 (27.4) | |
| Previous cystoscopies (n) | 0.598 | |||
| Mean±SD | 2.42±3.95 | 2.91±4.96 | 2.65±4.44 | |
| Range | 0-13 | 0-18 | 0-18 | |
| Type of cystoscope | 0.009 | |||
| Rigid | 8 (8.4) | 18 (18.9) | 26 (27.4) | |
| Flexible | 42 (44.2) | 27 (28.4) | 69 (72.6) | |
| Waiting time (min) | 0.211 | |||
| Mean±SD | 26.54±13.48 | 30.80±19.08 | 28.53±16.39 | |
| Range | 8-62 | 7-90 | 7-90 |
Values are presented as mean±standard deviation, mean (range), or a number (%) unless otherwise indicated.
SD: standard deviation.
Assessments by the patients following the intervention
| Music, n=50 | No music, n=45 | Total | p-value | |
|---|---|---|---|---|
| Procedure durationa) (min) | 0.847 | |||
| Mean±SD | 8.40±5.51 | 8.64±6.85 | 8.52±6.16 | |
| Range | 2-25 | 1-25 | 1-25 | |
| Discomfort (VAS) | 0.072 | |||
| Mean±SD | 26.88±21.77 | 35.89±25.65 | 31.24±24.03 | |
| Range | 0-70 | 0-100 | 0-100 | |
| Embarrassment (VAS) | 0.209 | |||
| Mean±SD | 29.27±28.26 | 37.11±31.28 | 33.06±29.86 | |
| Range | 0-100 | 0-100 | 0-100 | |
| Satisfaction (VAS) | 0.118 | |||
| Mean±SD | 78.13±18.14 | 70.56±27.47 | 74.46±23.31 | |
| Range | 40-100 | 0-100 | 0-100 | |
| Pain (VAS) | 0.613 | |||
| Mean±SD | 34.79±24.01 | 37.33±24.25 | 36.02±24.03 | |
| Range | 0-100 | 0-100 | 0-100 |
Values are presented as mean±standard deviation or mean (range).
SD: standard deviation, VAS: visual analogue scale.
a)Perceived procedure time by the patient.
Post-procedure patient assessments by the surgeon
| Music, n=50 | No music, n=45 | Total | p-value | |
|---|---|---|---|---|
| Procedure durationa) (min) | 0.047 | |||
| Mean±SD | 2.58±1.60 | 3.38±2.16 | 2.96±1.92 | |
| Range | 1-12 | 1-10 | 1-12 | |
| Discomfort (VAS) | 0.011 | |||
| Mean±SD | 24.17±18.40 | 30.33±13.66 | 27.15±16.49 | |
| Range | 0-80 | 10-60 | 0-80 | |
| Embarrassment (VAS) | 0.045 | |||
| Mean±SD | 26.04±19.10 | 34.00±18.63 | 29.89±19.19 | |
| Range | 0-90 | 10-70 | 0-90 | |
| Satisfaction (VAS) | 0.004 | |||
| Mean±SD | 77.40±13.60 | 69.11±13.28 | 73.39±14.01 | |
| Range | 30-100 | 30-100 | 30-100 | |
| Pain (VAS) | 0.020 | |||
| Mean±SD | 25.00±18.76 | 33.44±15.44 | 29.09±17.66 | |
| Range | 0-90 | 10-80 | 0-90 |
Values are presented as mean±standard deviation or mean (range).
SD: standard deviation, VAS: visual analogue scale.
a)Measured in real-time.
Summary of the periprocedural anxiety parameter and vital signs
| Music, n=50 | No music, n=45 | Total | p-value | |
|---|---|---|---|---|
| STAI-X-1 score, pre-procedural | 0.182 | |||
| Mean±SD | 37.44±9.60 | 40.04±9.27 | 38.67±9.48 | |
| Range | 20-59 | 20-58 | 20-59 | |
| STAI-X-1 score, post-procedural | 0.185 | |||
| Mean±SD | 36.40±10.30 | 39.2±9.92 | 37.75±10.16 | |
| Range | 20-60 | 20-60 | 20-60 | |
| Delta STAI-X-1 score | 0.871 | |||
| Mean±SD | 1.06±5.60 | 0.84±7.16 | 0.98±6.34 | |
| Range | -18 to 12 | -14 to 29 | -18 to 29 | |
| Precystoscopy HR (beats/min) | 0.837 | |||
| Mean±SD | 80.64±12.42 | 80.04±15.41 | 80.36±13.84 | |
| Range | 59-112 | 44-116 | 44-116 | |
| Postcystoscopy HR (beats/min) | 0.992 | |||
| Mean±SD | 80.92±13.42 | 80.89±13.37 | 80.90±13.32 | |
| Range | 60-119 | 54-110 | 54-119 | |
| Precystoscopy SBP (mmHg) | 0.603 | |||
| Mean±SD | 125.40±14.39 | 123.78±15.79 | 124.63±15.01 | |
| Range | 100-167 | 101-178 | 100-178 | |
| Postcystoscopy SBP (mmHg) | 0.621 | |||
| Mean±SD | 125.71±15.67 | 124.11±15.33 | 124.94±15.44 | |
| Range | 97-192 | 100-183 | 97-192 |
Values are presented as mean±standard deviation or mean (range).
STAI-X-1: State-Trait Anxiety Inventory-X-1, SD: standard deviation, HR: heart rate, SBP: systolic blood pressure.
Table 1
Patient characteristics and procedure details
Values are presented as mean±standard deviation, mean (range), or a number (%) unless otherwise indicated. SD: standard deviation.
Table 2
Assessments by the patients following the intervention
Values are presented as mean±standard deviation or mean (range). SD: standard deviation, VAS: visual analogue scale. a)Perceived procedure time by the patient.
Table 3
Post-procedure patient assessments by the surgeon
Values are presented as mean±standard deviation or mean (range). SD: standard deviation, VAS: visual analogue scale. a)Measured in real-time.
Table 4
Summary of the periprocedural anxiety parameter and vital signs
Values are presented as mean±standard deviation or mean (range). STAI-X-1: State-Trait Anxiety Inventory-X-1, SD: standard deviation, HR: heart rate, SBP: systolic blood pressure.

