


Articles
- Page Path
- HOME > Urogenit Tract Infect > Volume 17(3); 2022 > Article
- Original Article An Eight-Year Experience of Transvaginal Urethral Diverticulectomy: A Single-Center Study
-
Hyeon Woo Kim0
 , Jeong Zoo Lee0, Yangkyu Park1, Dong Gil Shin0
, Jeong Zoo Lee0, Yangkyu Park1, Dong Gil Shin0 -
Urogenital Tract Infection 2022;17(3):89-95.
DOI: https://doi.org/10.14777/uti.2022.17.3.89
Published online: December 31, 2022
Department of Urology, Pusan National University Hospital, Pusan National University School of Medicine, Busan
1Department of Mechanical Design Engineering, Chonnam National University, Yeosu, Korea
-
Correspondence to: Dong Gil Shin,https://orcid.org/0000-0002-9721-1706' target='_blank'> , Department of Urology, Pusan National University Hospital, Pusan National University School of Medicine, 179 Gudeok-ro, Seo-gu, Busan 49241, Korea, Tel: +82-51-240-7351, Fax: +82-51-247-5443, E-mail: shindong16@hanmail.net">shindong16@hanmail.net
• Received: August 16, 2022 • Revised: September 22, 2022 • Accepted: September 24, 2022
Copyright © 2022, Korean Association of Urogenital Tract Infection and Inflammation. All rights reserved.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 6,367 Views
- 13 Download
Abstract
-
Purpose This study aimed to analyze and report the surgical outcomes in female patients with urethral diverticulum (UD) over an eight-year period at a single center.
-
Materials and Methods Data of 49 UD females who underwent transvaginal urethral diverticulectomy between October 2011 and December 2019 were collected. The characterization of UD was reviewed using pelvic imaging studies. The pre- and post-operative symptoms, post-operative complications, and pathological findings were analyzed by reviewing the medical records.
-
Results The most frequent pre-operative symptom was dysuria (n=18), followed by incontinence (n=14), and these symptoms persisted until 3 months post-operatively in one and six patients, respectively. Pre-operative incontinence was cured in eight patients; however, de novo stress urinary incontinence occurred in five patients within a month after surgery. Submucosal macroplastique injection was administered to these patients; of whom, one was cured and three showed an improvement. Recurrent UD was found in seven patients at a mean of 14.14±17.21 months post-operatively, and a repeat diverticulectomy was performed in six of them; of these, one recurred again and was cured after the third diverticulectomy. Urethral strictures were observed in two patients within a month after the operation but improved after urethral dilatation. Bleeding and surgical site infections were observed in one and two patients, respectively, but were successfully managed conservatively. According to the pathological report, only one was diagnosed with urethral adenocarcinoma.
-
Conclusions Transvaginal urethral diverticulectomy can effectively manage UD, and its post-operative complications can be successfully managed by a proper treatment.
INTRODUCTION
Female urethral diverticulum (UD) is a rare disease with a worldwide prevalence rate ranging from 1% to 6% with unclear etiology [1,2]. The disease presents as a localized epithelium-lined outpouching of the urethra, located between the periurethral fibro-muscular layer and the anterior vaginal wall. Since the symptoms of UD are non-specific, the condition is often misdiagnosed as incontinence, recurrent urinary tract infection, lower urinary tract symptoms, which delay the proper management of the disease. UD is incidentally found in up to 1.4% of women who are tested for urinary incontinence, and in more than 80% of patients who present with periurethral masses [3,4].
The diagnosis and evaluation of UD are initiated by physical examinations of patients with a high index of suspicion of the disease. A palpable periurethral mass is found in more than half of the patients with UD [5]. On suspicion of UD based on physical examination, the diagnosis can be confirmed by cystourethroscopy and imaging modalities, such as balloon positive pressure urethrography, voiding cystourethrography, computerized tomography, ultrasound, or magnetic resonance imaging (MRI). Imaging studies are useful for evaluating the size, location, shape, and complexity of UD, and can be a blueprint for planning the course of treatment. Currently, the gold standard for diagnosis of UD is MRI, as it is the most appropriate technology for anatomic and tissue imaging assessment of UD, and provides invaluable information to plan the surgical procedure [6-8].
The current treatment of choice for female UD is transvaginal excision. It is reported to be the most effective treatment for managing UD, with high rates of success and low risk of complications [9-11]. However, the risk of potential complications following transvaginal urethral diverticulectomy, such as stress urinary incontinence (SUI), recurrence, and urethrovaginal fistula always exist, and patients need to be informed of these probable complications prior to surgery. There is a paucity of data on UD management due to the rarity of UD cases. As a result, decision-making presents a unique challenge in UD treatment. Thus, the present study sought to review the outcome data of the eight-year experience of using transvaginal urethral diverticulectomy, in female patients with UD and the incidence and management of post-operative complications at our institute.
MATERIALS AND METHODS
The present study retrospectively reviewed the electronic medical charts of women who underwent transvaginal urethral diverticulectomy without any other concomitant procedures from October 2011 to December 2019. A total of 49 UD patients without a history of prior urologic or gynecologic procedures who had at least 2-years post-operative follow-up medical records were included in the investigation. This study was approved by the Institutional Review Board of Pusan National University Hospital (No. 2109-008-107). Patient characteristics such as age at the time of surgery, symptoms associated with UD, and urological or gynecological history were investigated by chart review. The size, shape, and location of the UD of each patient were confirmed by reviewing pelvic imaging studies such as computed tomography (CT) or MRI scans. The size of the UD was estimated by measuring the maximal diameter of the diverticulum according to the transverse section of the images. The diverticular shape was classified as circumferential or simple depending on whether the urethra was encircled by the diverticulum or not, respectively. The UD was classified according to its location in the proximal and mid/distal portions of the urethra based on the sagittal section of the pelvic imaging studies.
According to the medical records of the included patients, all transvaginal urethral diverticulectomies were performed in a standard fashion [6] by a single surgeon (DGS). With the patient in the lithotomy position, an inverted U-shaped incision was made on the anterior vaginal wall at the level of the UD, followed by careful dissection around the diverticulum. Once the diverticulum was sufficiently exposed, complete excision of the UD followed by a watertight three-layer suture without tension was performed. Anti- incontinence procedures were not performed concomitantly during surgery. A 16-Fr urethral catheter was routinely maintained for at least a week post-operatively.
The remaining UD-related symptoms and the de novo symptoms after the surgery along with the pathological reports of the excised diverticulum were investigated by reviewing the follow-up medical records. In addition, the post-operative complications, complication-free period, and management of each type of complication along with their outcomes were reviewed. Continuous variables were described as mean±standard deviation and categorical variables as frequencies or proportions.
RESULTS
The mean age at the time of transvaginal urethral diverticulectomy, mean postoperative follow-up period of patients, and the mean maximal diameter of the UD were 52.71±9.53 years, 29.35±5.21 months, and 2.69±1.30 cm, respectively. Among the 49 patients, UD was diagnosed by CT and MRI in 23 and 26 patients, respectively. Since the CT scanner in our institute has a sufficiently high resolution, the UD could be easily defined in those evaluated by this imaging technique. According to the imaging studies, the UD was located at the mid/distal urethra in 27 (55.10%) and proximal urethra in 22 (44.90%) patients. Simple and circumferential UD was observed in 42 (85.71%) and seven (14.29%) patients, respectively (Table 1). Multiple instances of UD were reported in only one patient; the patient had two diverticula at the mid/distal urethra, and the maximal diameter of each diverticulum was 1 cm and 0.5 cm.
The most frequently reported UD-related symptom before the transvaginal urethral diverticulectomy was dysuria (n=18; 36.73%), followed by incontinence (n=14; 28.57%), pelvic pain (n=13; 26.53%), nocturia (n=11; 22.45%), vaginal mass (n=9; 18.37%), residual sensation (n=9; 18.37%), voiding difficulty (n=7; 14.29%), frequency (n=7; 14.29%), hematuria (n=7; 14.29%), and urgency to urinate (n=1; 2.04%). Asymptomatic UD, which was incidentally diagnosed by imaging studies such as CT and/or MRI, was observed in two (4.08%) patients (Fig. 1).
Pre-operative symptoms related to UD, such as dysuria (n=18), incontinence (n=14), vaginal mass (n=9), and frequency (n=7) persisted at three months after transvaginal urethral diverticulectomy in one (5.56%), six (42.86%), one (11.11%), and two (28.57%) patients, respectively. Post-operative de novo symptoms such as dysuria, incontinence, and voiding difficulty were observed in one (2.04%), five (10.20%), and two (4.08%) patients, respectively. The clinical symptoms of dysuria and voiding difficulty, which occurred post-surgery were caused by chronic inflammation at the surgical site and urethral stricture, respectively. Among the 14 patients who complained of incontinence before transvaginal urethral diverticulectomy, eight (57.14%) were cured after surgery (Fig. 1). According to the pathologic report of the UD tissue removed surgically, adenocarcinoma was diagnosed in one (2.04%) patient, and anterior pelvic exenteration with urinary diversion was performed as management of the condition.
Complications such as de novo SUI, recurrence of UD, mild urethral stricture, surgical site infection, and bleeding were observed after transvaginal urethral diverticulectomy. De novo SUI occurred in five (10.20%) patients within a month after surgery, and a submucosal macroplastique injection at the proximal urethra was administered to manage these patients. De novo SUI was cured in one (20%) patient and improved in three (60%) patients after the anti-incontinence procedure. The recurrence of UD was observed in seven (14.29%) patients at the mean of 14.14±17.21 months after the surgery. Repeat transvaginal urethral diverticulectomy was performed in six of these patients, while one patient refused further management. Among the six patients who underwent repeat surgery, five (83.33%) were cured, while UD recurred in one (16.67%) patient who was cured after a third transvaginal urethral diverticulectomy. A mild urethral stricture was present in two (4.08%) patients within a month after surgery, which improved after urethral dilatation using a Hegar dilator. Surgical site infections were observed in two (4.08%) patients and bleeding in one (2.04%) patient, within a month after the surgery. Patients with infection and bleeding were successfully managed with intravenous antibiotics and conservative management (Table 2).
DISCUSSION
According to our institutes’ eight-year experience of transvaginal urethral diverticulectomy, most of the symptoms related to UD improved after surgery. However, in a small proportion of patients, symptoms such as dysuria, incontinence, vaginal mass, and urinary frequency persisted at 3 months after transvaginal urethral diverticulectomy. Com-plications such as de novo SUI, recurrent UD, urethral stricture, surgical site infection, and bleeding occurred after the surgery in a small number of patients, and most of them improved with appropriate management. Pathological findings of the excised UD revealed urethral adenocarcinoma in one patient.
In our experience, the most frequently observed UD-related symptoms were dysuria (36.73%), incontinence (28.57%), and pelvic pain (26.53%). This result is similar to the classic triad of UD presentation, which is reported as the ‘3Ds’: dysuria, dyspareunia, and a dribble of urine after micturition [12]. Apart from dysuria which is one of the symptoms of the triad, incontinence and pelvic pain constitute the second and the third ‘D’s and can be matched to a dribble of urine after micturition and dyspareunia, respectively.
Transvaginal urethral diverticulectomy is the current treatment of choice for women with UD because of its high rate of success and low risk of post-operative complications [9-11]. In the present study, despite the results showing a high cure rate in most UD-related symptoms, a certain number of patients showed persistent dysuria (5.56%), incontinence (42.86%), vaginal mass (11.11%), and urinary frequency (28.57%) at 3 months following surgery. Our results indicate that the two common symptoms- incontinence and urinary frequency could not be resolved even after transvaginal urethral diverticulectomy in a majority of patients. This is attributed to the concomitant SUI and overactive bladder, respectively, which are considered unrelated to UD.
Concomitant SUI is one of the most frequently reported symptoms, occurring in approximately 10-57% of patients with UD[5,12-14]. Since SUI may disappear after urethral diverticulectomy in 50-100% of patients [15], clinicians are often ambivalent about their decision on whether to perform a concurrent anti-incontinence surgery or not [16]. Studies report that concurrent anti-incontinence surgery may have an advantage in preventing the need for a subsequent anti-incontinence procedure [7]. However, in the present study, not all patients with UD and concurrent incontinence underwent concurrent anti-incontinence surgery, primarily to avoid unnecessary procedural interventions and given the possibility of disappearance of SUI symptoms. In fact, more than half (57.14%) of the patients with UD and co-existing incontinence in our series showed resolution of incontinence after transvaginal urethral diverticulectomy. These patients included those with cessation of post-void dribbling as well as the disappearance of true SUI after surgery. A study in 2014 reported that concomitant SUI was resolved in 62% of patients with UD after urethral diverticulectomy [17], which was in line with our results.
Although transvaginal urethral diverticulectomy is an effective treatment option and is reported to have a high success rate of up to 97% [9-11], the risk of post-operative complications remains. In the present study, complications such as de novo SUI, recurrence of UD, mild urethral stricture, surgical site infection, and bleeding were observed in a small number of patients after transvaginal urethral diverticulectomy, and the occurrence rate of such complications was similar to that reported in other studies. De novo SUI after transvaginal urethral diverticulectomy was seen in 10.20% of the patients in our study, and this was found to be within the range of 1.7% to 33% reported by other studies [12,14,16,18-24]. The rates of UD recurrence and urethral stricture occurrence were 14.29% and 4.08%, respectively, and these rates were also within the range reported by other studies of 2-16% and 0-5.2%, respectively [7,14,17,24-26].
In our study, patients complaining of post-operative de novo SUI were managed by submucosal macroplastique injection at the proximal urethra, and 80% of them were cured or improved. Although post-operative de novo SUI may improve with time, up to 29% of the patients have been reported to require surgical treatment, such as a pubovaginal sling, Burch colposuspension, or urethral bulking agent injection [16]. Tension-free vaginal tape mid-urethral slings that can be successfully and safely placed have also been reported to be a treatment option [16]. However, synthetic slings can potentially increase the risk of diverticular recurrence, mesh erosion, and urethrovaginal fistula. Some studies have suggested that slings should be contraindicated for managing de novo SUI after urethral diverticulectomy [14,27]. The other post-operative complications that occurred in our study, such as recurrent UD, urethral stricture, and surgical site infection/bleeding, were all successfully managed by a repeat excision of UD, urethral dilatation, and conservative management. Additionally, placing a rectus fascia pubovaginal sling during repeat urethral diverticulectomy has been reported to be an effective method for decreasing the risk of further recurrence [28].
In our study, adenocarcinoma was diagnosed in one (2.04%) patient after transvaginal urethral diverticulectomy. The patient complained of hematuria prior to transvaginal urethral diverticulectomy, and there was no sign of malignancy on pre-operative CT images. According to other studies [29-31], 2-6% of female patients with UD presented with invasive carcinoma in their pathology report, and the results have shown that the majority of the malignancies were classified as adenocarcinoma. Diverticular malignancies may present with symptoms, such as hematuria, dysuria, urinary tract infection, and urinary obstruction [32]. There is no clear consensus regarding the management of urethral diverticular carcinoma due to its rarity and varied histology. Since there is a high risk of local recurrence and metastasis after a simple excision of the malignant UD, anterior pelvic exenteration with urinary diversion is usually recommended [29], which was also performed in our patient.
The present report has several limitations that need to be addressed. The number of subjects reviewed in the present study was low and they were all from only a single center. As a result, the data is insufficient for generalization. In addition, as the present study is a case series, its nature provided limits in the longitudinal data, and data regarding the outcomes after treatment were not standardized. Despite the limitations, the information in this study could support clinicians to determine a treatment plan for UD patients and the management of complications after urethral diverticulectomy. Larger multicenter cohort studies that can compensate for the aforementioned limitations are required to validate a clear and accurate medical course of treatment after the diagnosis of transvaginal urethral diverticulectomy and for the management of post-operative complications.
CONCLUSIONS
Transvaginal urethral diverticulectomy is an effective management procedure that significantly improves the presenting symptoms caused by UD. Although complications following transvaginal urethral diverticulectomy may be rare, they should be effectively managed with proper treatment as they may greatly impact the patient's quality of life. Also, given the enormous impact of these complications on the patient’s quality of life, patients should be informed of the probable complications and counseled on management options prior to the surgery. In the event of the occurrence of a complication, it should be appropriately managed, surgically or medically.
ACKNOWLEDGMENTS
This work was supported by a 2-year Research Grant of Pusan National University.
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
H.W.K. participated in data collection and wrote the manuscript. H.W.K. and Y.P. participated in the study design and performed the statistical analysis. J.Z.L. and D.G.S. participated in the study design and coordination and helped to draft the manuscript. All authors read and approved the final manuscript.
NOTES
Fig. 1
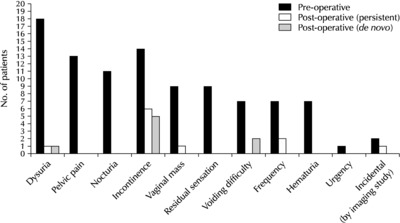
Presenting symptoms of female patients with urethral diverticulum before and after transvaginal urethral diverticulectomy.
Table 1
The location and type of urethral diverticulum in 49 patients included in the study
| Location | Type | Total | |
|---|---|---|---|
| Simple | Circumferential | ||
| Mid/distal urethra | 21 (42.86) | 6 (12.24) | 27 (55.10) |
| Proximal urethra | 21 (42.86) | 1 (2.04) | 22 (44.90) |
| Total | 42 (85.71) | 7 (14.29) | 49 (100) |
Table 2
Post-operative complications after transvaginal urethral diverticulectomy and their management
- 1. Davis BL, Robinson DG. Diverticula of the female urethra: assay of 120 cases. J Urol 1970;104:850-3. ArticlePubMed
- 2. Duchek M. Mårtensson O. Translabial ultrasonography with pulsed colour-Doppler in the diagnosis of female urethral diverticula. Scand J Urol Nephrol 1994;28:101-4. ArticlePubMed
- 3. Aldridge CW Jr, Beaton JH, Nanzig RP. A review of office urethroscopy and cystometry. Am J Obstet Gynecol 1978;131:432-7. ArticlePubMed
- 4. Blaivas JG, Flisser AJ, Bleustein CB, Panagopoulos G. Periurethral masses: etiology and diagnosis in a large series of women. Obstet Gynecol 2004;103(5 Pt 1):842-7. ArticlePubMed
- 5. Romanzi LJ, Groutz A, Blaivas JG. Urethral diverticulum in women: diverse presentations resulting in diagnostic delay and mismanagement. J Urol 2000;164:428-33. ArticlePubMed
- 6. Greenwell TJ, Spilotros M. Urethral diverticula in women. Nat Rev Urol 2015;12:671-80. ArticlePubMedPDF
- 7. Crescenze IM, Goldman HB. Female urethral diverticulum: current diagnosis and management. Curr Urol Rep 2015;16:71. ArticlePubMedPDF
- 8. Foster RT, Amundsen CL, Webster GD. The utility of magnetic resonance imaging for diagnosis and surgical planning before transvaginal periurethral diverticulectomy in women. Int Urogynecol J Pelvic Floor Dysfunct 2007;18:315-9. ArticlePubMedPDF
- 9. Hammad FT. TVT can also cause urethral diverticulum. Int Urogynecol J Pelvic Floor Dysfunct 2007;18:467-9. ArticlePubMedPDF
- 10. Tancer ML, Ravski NA. Suburethral diverticulum. Clin Obstet Gynecol 1982;25:831-7. ArticlePubMed
- 11. Shalev M, Mistry S, Kernen K, Miles BJ. Squamous cell carcinoma in a female urethral diverticulum. Urology 2002;59:773. Article
- 12. Ockrim JL, Allen DJ, Shah PJ, Greenwell TJ. A tertiary experience of urethral diverticulectomy: diagnosis, imaging and surgical outcomes. BJU Int 2009;103:1550-4. ArticlePubMed
- 13. Ganabathi K, Leach GE, Zimmern PE, Dmochowski R. Experience with the management of urethral diverticulum in 63 women. J Urol 1994;152(5 Pt 1):1445-52. ArticlePubMed
- 14. Ljungqvist L, Peeker R, Fall M. Female urethral diverticulum: 26-year followup of a large series. J Urol 2007;177:219-24. ArticlePubMed
- 15. Wilson A, Hussain M, Hamid R, Ockrim J, Shah J, Greenwel T, et al. Female urethral diverticula: evaluation of voiding dysfunction before and after surgery. J Urol 2012;187(4 Suppl):e630.
- 16. Stav K, Dwyer PL, Rosamilia A, Chao F. Urinary symptoms before and after female urethral diverticulectomy--can we predict de novo stress urinary incontinence? J Urol 2008;180:2088-90. ArticlePubMed
- 17. Reeves FA, Inman RD, Chapple CR. Management of symptomatic urethral diverticula in women: a single-centre experience. Eur Urol 2014;66:164-72. ArticlePubMed
- 18. Wharton LR Jr, Te Linde RW. Urethral diverticulum. Obstet Gynecol 1956;7:503-9.PubMed
- 19. Boatwright DC, Moore V. Suburethral diverticula in the female. J Urol 1963;89:581-4. ArticlePubMed
- 20. Ward JN. Technique to visualize urethral diverticula in female patients. Surg Gynecol Obstet 1989;168:278-9.PubMed
- 21. Porpiglia F, Destefanis P, Fiori C, Fontana D. Preoperative risk factors for surgery female urethral diverticula. Urol Int 2002;69:7-11. ArticlePubMedPDF
- 22. Lee UJ, Goldman H, Moore C, Daneshgari F, Rackley RR, Vasavada SP. Rate of de novo stress urinary incontinence after urethal diverticulum repair. Urology 2008;71:849-53. ArticlePubMed
- 23. Porten S, Kielb S. Diagnosis of female diverticula using magnetic resonance imaging. Adv Urol 2008;2008:213516. ArticlePubMedPMCPDF
- 24. Ingber MS, Firoozi F, Vasavada SP, Ching CB, Goldman HB, Moore CK, et al. Surgically corrected urethral diverticula: long-term voiding dysfunction and reoperation rates. Urology 2011;77:65-9. ArticlePubMed
- 25. Nickles SW, Ikwuezunma G, MacLachlan L, El-Zawahry A, Rames R, Rovner E. Simple vs complex urethral diverticulum: presentation and outcomes. Urology 2014;84:1516-9. ArticlePubMed
- 26. Han DH, Jeong YS, Choo MS, Lee KS. Outcomes of surgery of female urethral diverticula classified using magnetic resonance imaging. Eur Urol 2007;51:1664-70. ArticlePubMed
- 27. Vasavada SP. Urethral diverticula. Mosby; Philadelphia (PA): Article
- 28. Migliari R, Pistolesi D, D'Urso L, Muto G. Recurrent pseudo-diverticula of female urethra: five-year experience. Urology 2009;73:1218-22. ArticlePubMed
- 29. Thomas AA, Rackley RR, Lee U, Goldman HB, Vasavada SP, Hansel DE. Urethral diverticula in 90 female patients: a study with emphasis on neoplastic alterations. J Urol 2008;180:2463-7. ArticlePubMed
- 30. Pincus JB, Laudano M, Leegant A, Downing K. Female urethral diverticula: diagnosis, pathology, and surgical outcomes at an academic, urban medical center. Urology 2019;128:42-6. ArticlePubMed
- 31. Laudano MA, Jamzadeh AE, Dunphy C, Lee RK, Robinson BD, Tyagi R, et al. Pathologic outcomes following urethral diverti-culectomy in women. Adv Urol 2014;2014:861940. ArticlePubMedPMCPDF
- 32. Ahmed K, Dasgupta R, Vats A, Nagpal K, Ashrafian H, Kaj B, et al. Urethral diverticular carcinoma: an overview of current trends in diagnosis and management. Int Urol Nephrol 2010;42:331-41. ArticlePubMedPDF
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteAn Eight-Year Experience of Transvaginal Urethral Diverticulectomy: A Single-Center Study
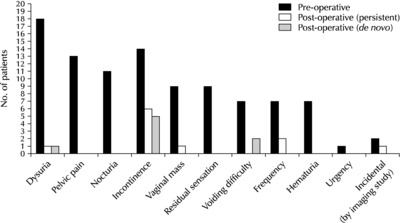
Fig. 1
Presenting symptoms of female patients with urethral diverticulum before and after transvaginal urethral diverticulectomy.
Fig. 1
An Eight-Year Experience of Transvaginal Urethral Diverticulectomy: A Single-Center Study
The location and type of urethral diverticulum in 49 patients included in the study
| Location | Type | Total | |
|---|---|---|---|
| Simple | Circumferential | ||
| Mid/distal urethra | 21 (42.86) | 6 (12.24) | 27 (55.10) |
| Proximal urethra | 21 (42.86) | 1 (2.04) | 22 (44.90) |
| Total | 42 (85.71) | 7 (14.29) | 49 (100) |
Values are presented as number (%).
Post-operative complications after transvaginal urethral diverticulectomy and their management
| Complications (Clavien–Dindo classification) |
n (%) | Complication-free period (mo) | Treatment (number of patients) |
|---|---|---|---|
| De novo stress urinary incontinence (Grade IIIa) | 5 (10.20) | <1 | Macroplastique injection (5) - Cured (1) - Improved (3) - Failed (1) |
| Recurrence (Grade IIIb) | 7 (14.29) | 14.14±17.21 (mean) | 1. Urethral diverticulectomy (6) - Cured (5) - 2nd recurrence (1): 3rd urethral diverticulectomy performed 2. Refused treatment (1) |
| Mild urethral stricture (Grade IIIa) | 2 (4.08) | <1 | Urethral dilatation using a Hegar dilator (2) - Improved (2) |
| Surgical site infection (Grade I) | 2 (4.08) | <1 | Intravenous antibiotics (2) - Cured (2) |
| Surgical site bleeding (Grade I) | 1 (2.04) | <1 | Conservative care (1) - Cured (1) |
Total number of patients who underwent transvaginal urethral diverticulectomy: 49.
Table 1
The location and type of urethral diverticulum in 49 patients included in the study
Values are presented as number (%).
Table 2
Post-operative complications after transvaginal urethral diverticulectomy and their management
Total number of patients who underwent transvaginal urethral diverticulectomy: 49.

