


Articles
- Page Path
- HOME > Urogenit Tract Infect > Volume 16(1); 2021 > Article
- Review Systematic Literature Review of the Urological Field and Considerations in COVID-19
-
Joongwon Choi
 , Hyun Soo Ryoo, Jae Hyun Ryu, Yun Beom Kim, Seung Ok Yang, Jeong Kee Lee, Tae Young Jung, Jung Hoon Kim1, Tae-Hyoung Kim2
, Hyun Soo Ryoo, Jae Hyun Ryu, Yun Beom Kim, Seung Ok Yang, Jeong Kee Lee, Tae Young Jung, Jung Hoon Kim1, Tae-Hyoung Kim2 -
Urogenital Tract Infection 2021;16(1):1-7.
DOI: https://doi.org/10.14777/uti.2021.16.1.1
Published online: April 30, 2021
Department of Urology, VHS Medical Center, Seoul, Korea
1Department of Urology, Hanil General Hospital, Seoul, Korea
2Department of Urology, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea
-
Correspondence to: Tae-Hyoung Kim,https://orcid.org/0000-0002-0257-3449' target='_blank'> , Department of Urology, Chung-Ang University Hospital, Chung-Ang University College of Medicine, 102 Heukseok‑ro, Dongjak‑gu, Seoul 06973, Korea, Tel: +82-2-6299-1818, Fax: +82-2-6299-2064, E-mail: kthlmk@nate.com">kthlmk@nate.com
• Received: March 31, 2021 • Revised: April 15, 2021 • Accepted: April 15, 2021
Copyright © 2021, Korean Association of Urogenital Tract Infection and Inflammation. All rights reserved.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,429 Views
- 1 Download
Abstract
- Coronavirus disease 2019 (COVID-19) was declared a worldwide pandemic in March 2020 after originating in China. Widespread uncertainty resulting from the pandemic has revolutionized urology practice worldwide, similar to that observed in other fields. The urological manifestations of COVID-19 were investigated by performing a literature search using a combination of keywords related to COVID-19 and urology. To date, COVID-19 has not been associated with any lower urinary tract symptoms, and there is no level 1 evidence that associates it with urinary malignancy and urolithiasis. Viral RNA has been detected in urine (5.74%), but there is no evidence of actual infection via urine. COVID-19 has transformed the standard urological practice into crisis-based care and has changed the medical and surgical priorities dramatically in the field. Most hospitals have established quarantine guidelines for each hospital, and procedures must be performed according to the present circumstances. Furthermore, in the absence of high-level evidence, specific efforts are needed to minimize the risk of COVID-19 infections during care.
INTRODUCTION
Coronavirus disease 2019 (COVID-19) has spread rapidly worldwide since November 2019 and has been touted as the “once-in-a-century pathogen we have always been worried about” [1]. Since the initial reports from China, COVID-19 progressed into a full-blown pandemic by March 2020 [2]. Before this, a Severe Acute Respiratory Syndrome (SARS)-Cov epidemic originating from China and a Middle East Respiratory Syndrome (MERS)-Cov epidemic originating from Saudi Arabia occurred from 2002 to 2003 and 2012, respectively. As of writing, the COVID-19 pandemic has affected most countries in the world. The coronavirus is an enveloped, single-stranded RNA virus with α, β, γ, and δ subtypes. The SARS-Cov-2 virus responsible for COVID-19 belongs to the β subtype and can maintain its viability at low temperatures because of its enveloped nature.
Widespread uncertainty caused by the pandemic has forced the urological field, as well as other medical fields, to adapt, and as a result, has revolutionized urology practice worldwide [3]. Hospitals face the massive challenge of providing ethical and quality care. This has affected urology practice and training and led to a decrease in the number of surgeries [4]. Indeed, this pandemic has resulted in a 20% decrease in urology referrals in the United States [5]. Furthermore, 93% of respondents in a previous study claimed that it affected their clinical practice of urology, with other reports claiming that the pandemic has severely decreased the quality of academic activities and residency training worldwide [6-8].
Hospitals have been forced to prioritize the quarantine system and have utilized various strategies to reduce the potential risks of COVID-19 infections among their staff [9]. These strategies include a screening test, which increases the workload of medical personnel, physicians, and other employees at increased risk of infection. Furthermore, a response strategy for COVID-19 has proven difficult to establish owing to its ongoing status and the lack of high-level evidence. This is compounded by issues, such as the claim by the Centers for Disease Control and Prevention, Unites States (CDC) that a new strain of COVID-19 was discovered in the United Kingdom at the end of 2020 [10].
Therefore, this paper evaluates the current situation of COVID-19 to provide information that would be helpful for the future of urology through a literature review related to COVID-19 and urology.
MAIN BODY
Publications on COVID-19 related to the urological field were reviewed systematically. A literature search was performed using a combination of keywords including ‘COVID- 19,’ ‘SARS-CoV-2,’ ‘Urology,’ ‘Urinary,’ and ‘Urological.’ The databases from MEDLINE, EMBASE, and the Cochrane library were searched for papers published until March 6, 2021. All returned articles were screened by one reviewer (J. Choi). To narrow the scope and improve the clarity of the manuscript’s contents, case reports, observational studies, non-randomized and randomized trials, and review articles on adult patients published in English were included in the literature review. Furthermore, information from organizations that published the latest news, including the CDC, World Health Organization (WHO), American Urological Association (AUA), and European Association of Urology (EAU) was also included. Fig. 1 presents the PRISMA flow diagram.
The coronavirus family Coronaviridae consists of approximately 42 types of enveloped, single-stranded RNA viruses. Most types infect only animal species, but some α and β subtypes, which SARS-CoV-2 belongs to, infect humans [11].
COVID-19 is spread through person-to-person contact, mainly through aerosols, and has also been reported to be transmitted through physical contact of fomites, such as contaminated water purifiers [2]. The common symptoms of COVID-19 include dry cough, fever, shortness of breath, fatigue, and loss of appetite. Pneumonia can develop in severe cases, which may require ventilatory support. In vivo invasion of the virus occurs via the attachment of a virus spike protein to the angiotensin-converting enzyme 2 (ACE2) receptor in the lungs, liver, intestines, heart, kidney, bladder, testis, and brain. The virus is then internalized by the transmembrane serine proteinase 2 (TMPRSS2) gene. The virus has been detected in the throat, feces, blood, and urine and the reported incubation ranges from two to 14 days [12]. Viral RNA for COVID-19 is collected via a nasopharyngeal and oropharyngeal swab and has been found in fecal (65.8%), blood (low), and urine (5.74%) specimens. No solid data for semen specimens are available [13]. Although virus RNA is detected in urine, it is unknown if COVID-19 is transmitted through urine or how long the virus RNA has been shedding. COVID-19 has a lower mortality rate than MERS-Cov (3.4% vs. 35%) but higher transmissibility [14].
According to the CDC, various diseases have caused widespread damage to public health. Examples include polio in 1955, smallpox in 1966, and anthrax in 2001, and more recently, epidemics, such as SARS in 2003 and the Zika virus in 2016. The death toll of COVID-19 has already passed that from the Hong-Kong flu, swine flu, and yellow fever [15-18]. In contrast, the death toll is not as high as that of cholera, the Black Death, and smallpox (Fig. 2). According to the WHO, more than 115,000,000 people have been infected and more than 2,500,000 have died by March 2021 [19]. According to the WHO data on 237 countries last updated in March 2021, the United States of America had the highest number of cases and deaths. The Republic of Korea ranked 86th for total cases with 91,240 cases, 165th for cases per 100,000 people, and 86th for mortalities with 1,619 deaths (Table 1). COVID-19 has transformed the standard urological practice into crisis-based care that has decreased the number of operations performed in the hospital [4,20].
Regarding sex and the status of COVID-19, male COVID-19 patients were reported to have greater severity of illness and a higher mortality rate [21]. In December 2020, the number of cases was similar in both sexes, but the death toll was approximately 36% higher for males. This may be due to the larger number of ACE2 receptors in the lungs and heart of males [12]. Additionally, androgens can reduce immunity. Finally, smoking is a known risk factor for respiratory infections.
1) General considerations
No level 1 evidence regarding COVID-19 exists in the urologic field. Most papers were based on level 3 evidence or expert opinions, such as the actual urgency of each diagnostic or therapeutic procedure and the tradeoff between the available resources and the risks of deferring elective interventions [3].
The possibility of viral cystitis was initially reported in March 2020 [22]. Urosepsis cases that were then diagnosed with COVID-19, an increase in urinary frequency pre- and post-treatment (13.7/day) was observed in seven out of 57 males (12.3%). On the other hand, given that the symptoms worsened since the initial diagnosis of urosepsis, it may be insufficient to infer that an increase in frequency is a symptom of COVID-19. This case series may have erroneously inferred this because it was published early during the COVID-19 pandemic. Regarding the potential mode of action, the ACE2 receptor has been reported to act as a receptor for COVID-19 [23]. This leads to the possibility of infection of urothelial cells. Furthermore, infection through urine may be possible because some reports have found viral RNA in urine.
Considering the subsequent papers on COVID-19, the virus is unlikely to cause any urinary symptoms. The presence of urinary symptoms alone should not raise any significant concerns of COVID-19. On the other hand, a high level of suspicion of COVID-19 may be needed if a patient presents with fever in addition to the urinary symptoms. One paper published during the COVID-19 pandemic suggested that patients showed more critical and demanding urological manifestations in the emergency department [24].
There are several concerns of potential COVID-19 infections during procedures and standard medical practice. First, viral shedding in stools can persist for up to six weeks after the onset of symptoms. Thus, utilizing the transrectal approach during a pandemic may carry a potential infection risk [13]. Therefore, when COVID-19 is suspected, proper utilization of personal protective equipment must be observed despite the lack of reports of fecal–oral transmission of COVID-19 [11]. Second, laparoscopy can result in a high gas concentration in the abdomen and cause viral aerosolization [25]. Third, specimens associated with COVID-19 must be carried in non-leaking bags or containers. Hence, pathologists must use the appropriate protective equipment, including glasses, a medical mask, sleeves, gloves, a laboratory coat, and specific aprons. Furthermore, viral residue may remain on glass and plastic surfaces for up to nine days [26].
2) Acute kidney injury in COVID-19
In COVID-19 patients, the reported prevalence of acute kidney injury was 7.58% [12]. This has been reported as a possible manifestation of COVID-19 and suggests a more serious disease [27]. Although the mechanism is unclear, ACE2 receptors at the proximal convoluted tubules may be at high risk of viral invasion [11]. Acute kidney injury requires continuous renal replacement therapy, and the mortality rate is 93.3% [20].
3) Urological guidelines of COVID-19
The EAU released COVID-19 recommendations last April 2020 [28], with the last update released last January 2021. The paper assigned surgical patients into four priority levels described below, and only those of high priority and emergency cases could undergo surgery. Additionally, there are currently no high-quality reports, and there may be significant differences between countries and regions.
Low priority: clinical harm very unlikely if postponed for six months
Intermediate priority: clinical harm possible, but unlikely, if postponed for three-four months
High priority: clinical harm very likely if postponed for >six weeks
Emergency: life-threatening situation – cannot be postponed for >24 hours
AUA currently operates the COVID-19 information center [29]. Information regarding vaccines and various clinical insights about the urological field was updated every week. Most reports are related to early experience or telehealth, and there are little data on the urological oncological practice during the COVID-19 pandemic. During the pandemic, an argument claimed that patients preferred telemedicine to face-to-face consultation beyond the physician’s requirements [30-32]. BJU International also runs blogs on the urological aspects of COVID-19 [33].
(1) Renal cancer in COVID-19: Thus far, no high-level evidence regarding any direct correlation between urological tumors and COVID-19 exists [34]. On the other hand, some recommendations regarding situations where the potential infection risk and burdens on the medical staff are increased. The CCAFU recommended the treatment of renal cancer during the COVID-19 pandemic as follows:
T1-T2: postponed under supervision
T3- and symptomatic tumor: surgery
Cytoreductive nephrectomy: decision according to the prognostic stage, monitoring, or medical treatment
(2) Bladder cancer in COVID-19: Data on the treatment of patients with Bacillus Calmette-Güérin (BCG) for bladder cancer and whether there is an increased risk of COVID-19 infection are currently limited. Moreover, it is unclear if the caregiver administering BCG treatment is at risk of contracting an infection from the COVID-19 patient. Thus far, in COVID-19 patients with non-muscle invasive bladder cancer, the installation of BCG is recommended to be delayed for at least three weeks after the initial symptoms in both the induction and maintenance period [35]. Nonsteroidal anti-inflammatory drugs (NSAID) are commonly used to control the symptoms in BCG-treated patients. On the other hand, they should only be used in patients with no COVID-19 infection because they may lead to a higher risk of hospital-ization and intensive care unit admission. Furthermore, there are some ongoing clinical trials on the use of BCG as a possible prophylactic vaccine against COVID-19 [36].
(3) Prostate cancer in COVID-19: A recent study reported that prostate cancer patients who received androgen deprivation therapy had a higher risk of COVID-19 infection [37]. In metastatic castration-resistant prostate cancer, the expression of the androgen receptor and TMPRSS2 were positively correlated. More androgens may increase the expression of TMPRSS2, which may lead to increased susceptibility to COVID-19. Nevertheless, this was not included in the National Comprehensive Cancer Network (NCCN) recommendations on prostate cancer management of COVID-19 patients [38].
(4) Stones in COVID-19: Urinary stone management accounts for up to 30% of the daily practice of a general urologist [39]. During the pandemic, stone patients were separated into those who could be delayed from those who could not [40]. The de-escalation of surgical activity has resulted in the treatment of emergency cases. A non-obstructing renal stone should be treated with low priority. The preferential cases were as follows: stones in a solitary kidney, acute kidney injury status, bilateral obstruction, and severe pain. In contrast, non-obstructing stones and ureteral stent removal should be rescheduled [41].
Most guidelines focused on delaying treatment by prioritizing the cases based on level 3 evidence or expert opinions. The establishment of a database of delayed treatments and surgeries is essential to understanding the possible effects on safety and outcome [42].
CONCLUSIONS
The COVID-19 pandemic has seriously threatened public health and has drastically changed medical and surgical priorities worldwide. Most hospitals have established guidelines on quarantine and what procedures must be performed according to the circumstances. Furthermore, it has become necessary to develop guidelines in the absence of high-level evidence to minimize the risk of COVID-19 infection during procedures and care. At the very least, efforts are needed to reduce the number of aerosol-generating procedures.
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
J.C. and T.H.K. participated in data collection and wrote the manuscript. H.S.R., J.H.R., J.H.K., and Y.B.K. participated in the study design and performed the statistical analysis. S.O.Y., J.K.L., and T.Y.J. participated in the study design and coordination and helped to draft the manuscript. All authors read and approved the final manuscript.
NOTES
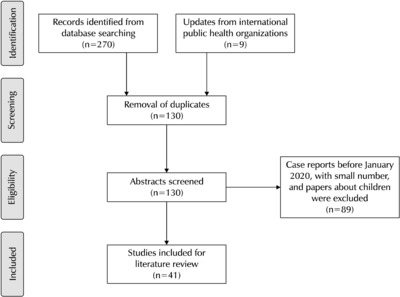
Fig. 2
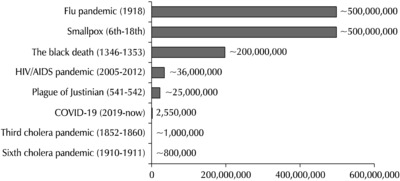
Pandemic deaths through history. Available from: https://www.who.int/emergencies/diseases/en/. COVID-19: corona-virus disease 2019.
Table 1
WHO COVID-19 global data (2021. 3 update)
Available from: https://covid19.who.int/.
WHO: World Health Organization, COVID-19: coronavirus disease 2019.
- 1. Nowroozi A, Amini E. Urology practice in the time of COVID-19. Urol J 2020;17:326.PubMed
- 2. Ahmed K, Hayat S, Dasgupta P. Global challenges to urology practice during the COVID-19 pandemic. BJU Int 2020;125:E5-6. ArticlePubMedPMCPDF
- 3. Amparore D, Campi R, Checcucci E, Sessa F, Pecoraro A, Minervini A, et al. Forecasting the future of urology practice: a comprehensive review of the recommendations by International and European Associations on priority procedures during the COVID-19 pandemic. Eur Urol Focus 2020;6:1032-48. ArticlePubMedPMC
- 4. Yee CH, Wong HF, Tam MHM, Yuen SKK, Chan HC, Cheung MH, et al. Feb 26 Effect of SARS and COVID-19 outbreaks on urology practice and training. Hong Kong Med J 2021;[Epub]. DOI: 10.12809/hkmj208822. Article
- 5. Lewicki P, Basourakos SP, Al Awamlh BAH, Wu X, Hu JC, Schlegel PN, et al. Estimating the impact of COVID-19 on urology: data from a large nationwide cohort. Eur Urol Open Sci 2021;25:52-6. ArticlePubMedPMC
- 6. Amparore D, Claps F, Cacciamani GE, Esperto F, Fiori C, Liguori G, et al. Impact of the COVID-19 pandemic on urology residency training in Italy. Minerva Urol Nefrol 2020;72:505-9. ArticlePubMed
- 7. Dotzauer R, Böhm K, Brandt MP, Sparwasser P, Haack M, Frees SK, et al. Jul 4 Global change of surgical and oncological clinical practice in urology during early COVID-19 pandemic. World J Urol 2020;[Epub]. DOI: 10.1007/s00345-020-03333-6. ArticlePDF
- 8. Heinze A, Umari P, Basulto-Martínez M, Suárez-Ibarrola R, Liatsikos E, Rassweiler J, et al. Impact of COVID-19 on clinical and academic urological practice: a survey from European Association of Urology section of uro-technology. Eur Urol Open Sci 2020;21:22-8. ArticlePubMedPMC
- 9. Choi SY, Kim TH. Survival strategy of urology department during the COVID-19 era. Int Urol Nephrol 2020;52:1499-500. ArticlePubMedPMCPDF
- 10. Centers for Disease Control and Prevention (CDC). About variants of the virus that causes COVID-19 [Internet]. Atlanta: CDC; 2021 [cited 2021 Mar 15]. Available from: https://www.cdc.gov/coronavirus/2019-ncov/transmission/variant.html
- 11. Puliatti S, Eissa A, Eissa R, Amato M, Mazzone E, Dell'Oglio P, et al. COVID-19 and urology: a comprehensive review of theliterature. BJU Int 2020;125:E7-14. ArticlePubMedPDF
- 12. Chan VW, Chiu PK, Yee CH, Yuan Y, Ng CF, Teoh JY. May 27 A systematic review on COVID-19: urological manifestations, viral RNA detection and special considerations in urological conditions. World J Urol 2020;[Epub]. DOI: 10.1007/s00345- 020-03246-4. ArticlePDF
- 13. Peng L, Liu J, Xu W, Luo Q, Chen D, Lei Z, et al. SARS-CoV-2can be detected in urine, blood, anal swabs, and oropharyngeal swabs specimens. J Med Virol 2020;92:1676-80. ArticlePubMedPMCPDF
- 14. Desouky E. COVID-19 impact on urology practice: a possible dilemma of misdiagnosis. Arab J Urol 2020;18:59-61. ArticlePubMedPMC
- 15. World Health Organization (WHO). WHO report on global surveillance of epidemic-prone infectious diseases [Internet]. Geneva: WHO; c2000 [cited 2021 Mar 15]. Available from: https://www.who.int/csr/resources/publications/surveillance/plague.pdf
- 16. World Health Organization (WHO). Disease outbreaks [Internet]. Geneva: WHO; 2021 [cited 2021 Mar 15]. Available from: https://www.who.int/emergencies/diseases/en/
- 17. World Health Organization (WHO). Ebola virus disease [Internet]. Geneva: WHO; 2021 [cited 2021 Mar 15]. Available from: https://www.who.int/news-room/fact-sheets/detail/ebola-virus-disease
- 18. World Health Organization (WHO). Influenza: data and statistics [Internet]. Geneva: WHO; 2021 [cited 2021 Mar 15]. Available from: https://www.euro.who.int/en/health-topics/communicable-diseases/influenza/data-and-statistics
- 19. World Health Organization (WHO). WHO coronavirus (COVID-19) dashboard [Internet]. Geneva: WHO; 2021 [cited 2021 Mar 15]. Available from: https://covid19.who.int/
- 20. Thapa BB, Shrestha D, Bista S, Thapa S, Niranjan V. Urology during COVID-19 pandemic crisis: a systematic review. Surg J (N Y) 2021;7:e3-10. ArticlePubMedPMC
- 21. Jin P, Park H, Jung S, Kim J. Challenges in urology during the COVID-19 pandemic. Urol Int 2021;105:3-16. ArticlePubMedPDF
- 22. Mumm JN, Osterman A, Ruzicka M, Stihl C, Vilsmaier T, Munker D, et al. Urinary frequency as a possibly overlooked symptom in COVID-19 patients: does SARS-CoV-2 cause viral cystitis? Eur Urol 2020;78:624-8. ArticlePubMedPMC
- 23. Fan C, Lu W, Li K, Ding Y, Wang J. ACE2 expression in kidney and testis may cause kidney and testis infection in COVID-19 patients. Front Med 2017;563893. Article
- 24. Gallioli A, Albo G, Lievore E, Boeri L, Longo F, Spinelli MG, et al. How the COVID-19 wave changed emergency urology: results from an academic tertiary referral hospital in the epicentre of the Italian red zone. Urology 2021;147:43-9. ArticlePubMed
- 25. Chiancone F, Fedelini P. Managing change in the urology department of a large hospital in Italy during the COVID-19 pandemic. Int J Urol 2020;27:820-2. ArticlePubMedPMCPDF
- 26. Compérat E. What does COVID-19 mean for the pathology- urology interaction? Eur Urol 2020;78:e43-4. ArticlePubMedPMC
- 27. Cheng Y, Luo R, Wang K, Zhang M, Wang Z, Dong L, et al. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int 2020;97:829-38. ArticlePubMedPMC
- 28. European Association of Urology (EAU). COVID-19 recom-mendations [Internet]. Arnhem: EAU; c2020 [cited 2021 Mar 15]. Available from: https://uroweb.org/guideline/covid-19-recommendations/
- 29. American Urological Association (AUA). COVID-19 info center [Internet]. Linthicum Heights: AUA; 2021 [cited 2021 Mar 15]. Available from: https://www.auanet.org/covid-19-info-center/covid-19-info-center
- 30. Boehm K, Ziewers S, Brandt MP, Sparwasser P, Haack M, Willems F, et al. Telemedicine online visits in urology during the COVID-19 pandemic-potential, risk factors, and patients' perspective. Eur Urol 2020;78:16-20. ArticlePubMedPMC
- 31. Borchert A, Baumgarten L, Dalela D, Jamil M, Budzyn J, Kovacevic N, et al. Managing urology consultations during COVID-19 pandemic: application of a structured care pathway. Urology 2020;141:7-11. ArticlePubMed
- 32. Novara G, Checcucci E, Crestani A, Abrate A, Esperto F, Pavan N, et al. Research Urology Network (RUN). Telehealth in urology: a systematic review of the literature. How much can telemedicine be useful during and after the COVID-19 pandemic? Eur Urol 2020;78:786-811. PubMedPMC
- 33. Dasgupta P. Covid-19 and urology. BJU Int 2020;125:749. ArticlePubMedPMCPDF
- 34. Zequi SC, Abreu D. Consideration in the management of renal cell carcinoma during the COVID-19 Pandemic. Int Braz J Urol 2020;46(Suppl 1):69-78. ArticlePubMedPMC
- 35. Lenfant L, Seisen T, Loriot Y, Rouprêt M. Adjustments in the use of intravesical instillations of bacillus Calmette-Guérin for high-risk non-muscle-invasive bladder cancer during the COVID-19 pandemic. Eur Urol 2020;78:1-3. ArticlePubMedPMC
- 36. Desouky E. BCG versus COVID-19: impact on urology. World J Urol 2021;39:823-7. ArticlePubMedPDF
- 37. Montopoli M, Zumerle S, Vettor R, Rugge M, Zorzi M, Catapano CV, et al. Androgen-deprivation therapies for prostate cancer and risk of infection by SARS-CoV-2: a population-based study (N = 4532). Ann Oncol 2020;31:1040-5. ArticlePubMed
- 38. National Comprehensive Cancer Network (NCCN). Management of prostate cancer during the COVID-19 pandemic [Internet]. Plymouth: NCCN; c2020 [cited 2021 Mar 15]. Available from: https://www.nccn.org/covid-19/pdf/NCCN_PCa_COVID_guidelines.pdf
- 39. Mazzucchi E, Torricelli FCM, Vicentini FC, Marchini GS, Danilovic A, Batagello CA, et al. The impact of COVID-19 in medical practice. A review focused on urology. Int Braz J Urol 2021;47:251-62. ArticlePubMedPMC
- 40. Proietti S, Gaboardi F, Giusti G. Endourological stone management in the era of the COVID-19. Eur Urol 2020;78:131-3. ArticlePubMedPMC
- 41. Heldwein FL, Loeb S, Wroclawski ML, Sridhar AN, Carneiro A, Lima FS, et al. A systematic review on guidelines and recommendations for urology standard of care during the COVID-19 pandemic. Eur Urol Focus 2020;6:1070-85. ArticlePubMedPMC
- 42. Margel D, Ber Y. 2020 May 13 Changes in urology after the first wave of the COVID-19 pandemic. Eur Urol Focus. [Epub]. DOI: 10.1016/j.euf.2020.05.001. Article
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteSystematic Literature Review of the Urological Field and Considerations in COVID-19
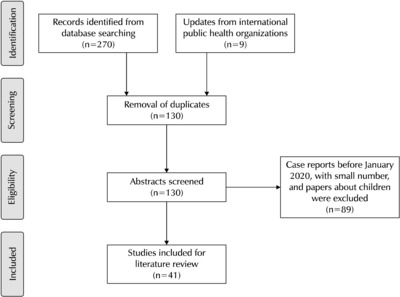
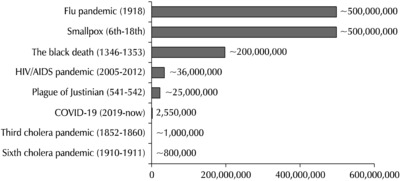
Fig. 1
PRISMA flow diagram.
Fig. 2
Pandemic deaths through history. Available from: https://www.who.int/emergencies/diseases/en/. COVID-19: corona-virus disease 2019.
Fig. 1
Fig. 2
Systematic Literature Review of the Urological Field and Considerations in COVID-19
WHO COVID-19 global data (2021. 3 update)
| Country name | Cases - cumulative total | Rank | Cases - total per 100,000 population | Rank | Deaths - cumulative total | Rank |
|---|---|---|---|---|---|---|
| Global | 114,853,685 | 1,471.3 | 2,554,694 | |||
| United States | 28,403,416 | 1 | 8,581.0 | 9 | 513,071 | 1 |
| India | 11,156,923 | 2 | 808.5 | 128 | 157,435 | 4 |
| Brazil | 10,646,926 | 3 | 5,008.9 | 40 | 257,361 | 2 |
| Russian Federation | 4,290,135 | 4 | 2,939.8 | 75 | 87,823 | 7 |
| The United Kingdom | 4,194,789 | 5 | 6,179.2 | 26 | 123,783 | 5 |
| France | 3,744,060 | 6 | 5,736.0 | 30 | 87,093 | 8 |
| Spain | 3,136,321 | 7 | 6,708.0 | 19 | 70,247 | 10 |
| Italy | 2,976,274 | 8 | 4,922.6 | 41 | 98,635 | 6 |
| Turkey | 2,734,836 | 9 | 3,242.7 | 67 | 28,771 | 20 |
| Germany | 2,471,942 | 10 | 2,950.4 | 73 | 71,240 | 9 |
| Republic of Korea | 91,240 | 86 | 178.0 | 165 | 1,619 | 86 |
Available from:
WHO: World Health Organization, COVID-19: coronavirus disease 2019.
Table 1
WHO COVID-19 global data (2021. 3 update)
Available from: WHO: World Health Organization, COVID-19: coronavirus disease 2019.

