


Search
- Page Path
- HOME > Search
Original Article
- The Korean Antimicrobial Resistance Monitoring System for Complicated Urinary Tract Infections: A Prospective Multicenter Observational Study Conducted by the Korean Association of Urogenital Tract Infection and Inflammation
- Seong Hyeon Yu, Seung Il Jung, Donghoon Lim, Jeong Woo Lee, Seung-Ju Lee, Hong Chung, Mi-Mi Oh, Jing Bong Choi, Jae Hung Jung, Hee Jo Yang, KAUTII Investigators
- Urogenit Tract Infect 2026;21(1):15-25. Published online April 30, 2026
- DOI: https://doi.org/10.14777/uti.2550040020
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader - Purpose
This study aimed to report antimicrobial resistance (AMR) patterns among patients with complicated urinary tract infection (cUTI) using data from the Korean Antimicrobial Resistance Monitoring System (KARMS). Materials and Methods: In this prospective, multicenter, observational surveillance study, data from patients diagnosed with cUTI between January 2023 and September 2025 were retrieved from the KARMS database. Demographic characteristics, uropathogen distribution, and antimicrobial susceptibility profiles of representative pathogens were analyzed.
Results
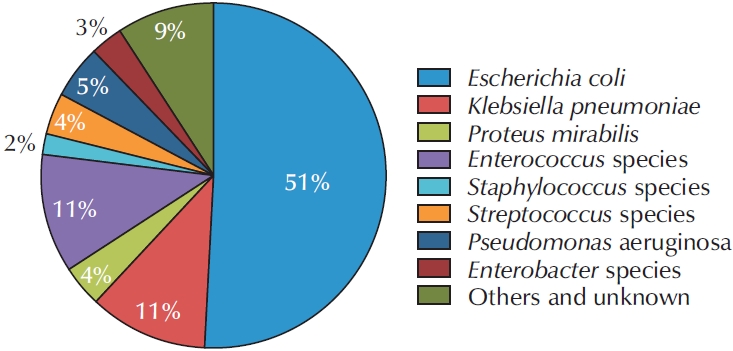
Data from a total of 698 patients were collected in the KARMS database. The mean patient age was 68.94±15.95 years. The numbers of patients with healthcare-associated UTI and recurrent UTI were 171 (24.5%) and 240 (34.4%), respectively. Escherichia coli was the most frequently identified uropathogen (n=356, 51.1%). Regarding antimicrobial susceptibility, 92.9% of isolates were susceptible to fosfomycin, 75.5% to nitrofurantoin, 47.2% to ciprofloxacin, 63.3% to cefotaxime, 80.6% to piperacillin/tazobactam, and 98.8% to ertapenem. The rate of extended-spectrum beta-lactamase positivity was 45.2% (166 of 367) and was significantly higher in pyelonephritis and urosepsis (62.3% and 62.5%, p=0.002), healthcare-associated UTI (58.6%, p=0.040), and recurrent cUTI (53.2%, p=0.028). Fluoroquinolone resistance was significantly more common in female patients (49.1%, p=0.021) and in healthcare-associated UTI (57.9%, p=0.014). Piperacillin/tazobactam resistance was significantly higher in patients with urosepsis (37.0%, p=0.004), in tertiary hospitals (17.2%, p=0.019), and in healthcare-associated UTI (26.4%, p=0.001). In addition, third-generation cephalosporin resistance was significantly higher in secondary hospitals than in tertiary hospitals (43.5% vs. 33.3%, p=0.041).
Conclusions
These data provide current information on uropathogen distribution and AMR patterns in cUTI in South Korea. Continued surveillance and ongoing data accumulation through KARMS will support evidence-based strategies for optimal antimicrobial therapy and AMR mitigation.
- 937 View
- 26 Download

Review Articles
- Molecular Mechanisms of Antibiotic Resistance in Uropathogenic Escherichia coli: A Narrative Review
- Nakjun Choi, Dong Uk Kim, Eun-Jin Lee
- Urogenit Tract Infect 2025;20(2):96-106. Published online August 31, 2025
- DOI: https://doi.org/10.14777/uti.2550018009
-
Abstract
PDFPubReader
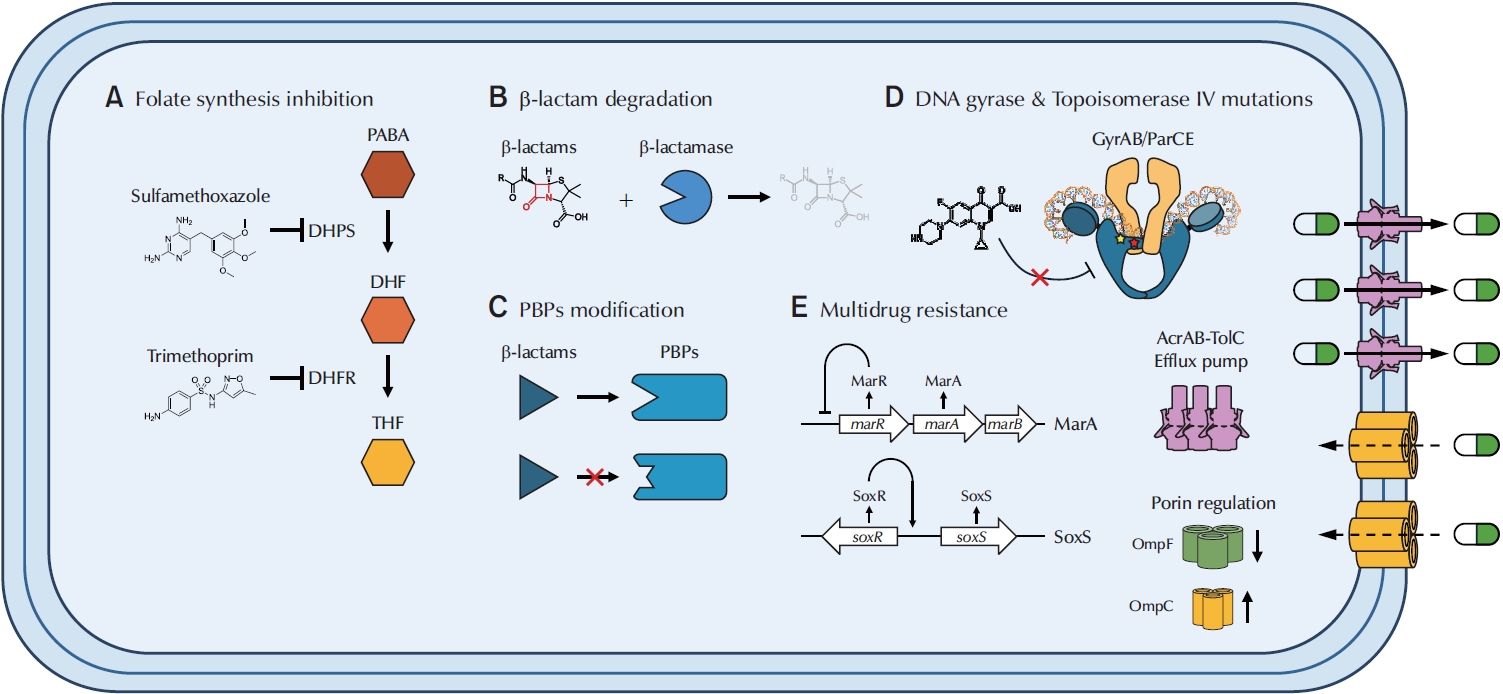
- Urinary tract infections (UTIs) are among the most prevalent bacterial infections worldwide, with uropathogenic Escherichia coli (UPEC) serving as the primary causative agent. Although antibiotic therapy remains the standard of care for UTI treatment, the increasing prevalence of antimicrobial resistance has substantially reduced the effectiveness of commonly prescribed antibiotics. Resistance to trimethoprim-sulfamethoxazole (TMP-SMX), β-lactams, and fluoroquinolones is particularly concerning, as these agents constitute the principal therapeutic options for UTIs. This review examines the molecular mechanisms underlying UPEC resistance to these three classes of antibiotics, including target site modifications, efflux pump overexpression, porin regulation, and enzymatic degradation. Furthermore, it explores how these resistance determinants contribute to the development of multidrug-resistant (MDR) UPEC strains, which demonstrate cross-resistance to multiple antibiotics and present significant challenges for clinical management. Novel therapeutic strategies, such as efflux pump inhibitors, bacteriophage therapy, and genomic-guided precision medicine, are under investigation as potential solutions to address the growing global burden of MDR UPEC, alongside alternative non-antibiotic treatments. This review aims to provide a comprehensive overview of the genetic and regulatory pathways driving antibiotic resistance in UPEC, offering insights that may guide the development of effective treatment strategies and help mitigate the ongoing spread of antimicrobial resistance.
-
Citations
Citations to this article as recorded by
- Biological mechanisms and social determinants of antimicrobial resistance
Madhulika Bajpai, Tanisha Saraf, Urmi Bajpai
Biochemical and Biophysical Research Communications.2026; 828: 154075. CrossRef -
Phenotypic and molecular evaluation of efflux pump activity and biofilm formation in clinical MDR
Klebsiella pneumoniae
isolates
Samaa Sameh Bakr, Dina Eid Rizk, El Sayed E. Habib, Enas Yasser Sultan
Egyptian Journal of Basic and Applied Sciences.2026; 13(1): 251. CrossRef - Rapid diagnostics innovations for urinary tract infections using molecular biology, artificial intelligence and antimicrobial resistance surveillance: a comprehensive review
Soniya Goyal, Pooja Sharma, Deepak Aggarwal, Sameer Singh Faujdar
Molecular Biology Reports.2026;[Epub] CrossRef - Editorial for Urogenital Tract Infection (UTI) 2025 Vol. 20 No. 2 – Highlights of This Issue’s Papers and the UTI Editors’ Pick
Koo Han Yoo
Urogenital Tract Infection.2025; 20(2): 55. CrossRef
- Biological mechanisms and social determinants of antimicrobial resistance
- 10,823 View
- 237 Download
- 4 Crossref
- Beta-Lactamase-Mediated Antibiotic Resistance in Urinary Tract Infections: Mechanisms and Therapeutic Strategies
- Fanglin Shao, Dengxiong Li, Jie Wang, Zhouting Tuo, Zhipeng Wang, Wuran Wei, Ruicheng Wu, Dechao Feng
- Urogenit Tract Infect 2025;20(2):67-81. Published online August 31, 2025
- DOI: https://doi.org/10.14777/uti.2550012006
-
Abstract
PDFPubReader
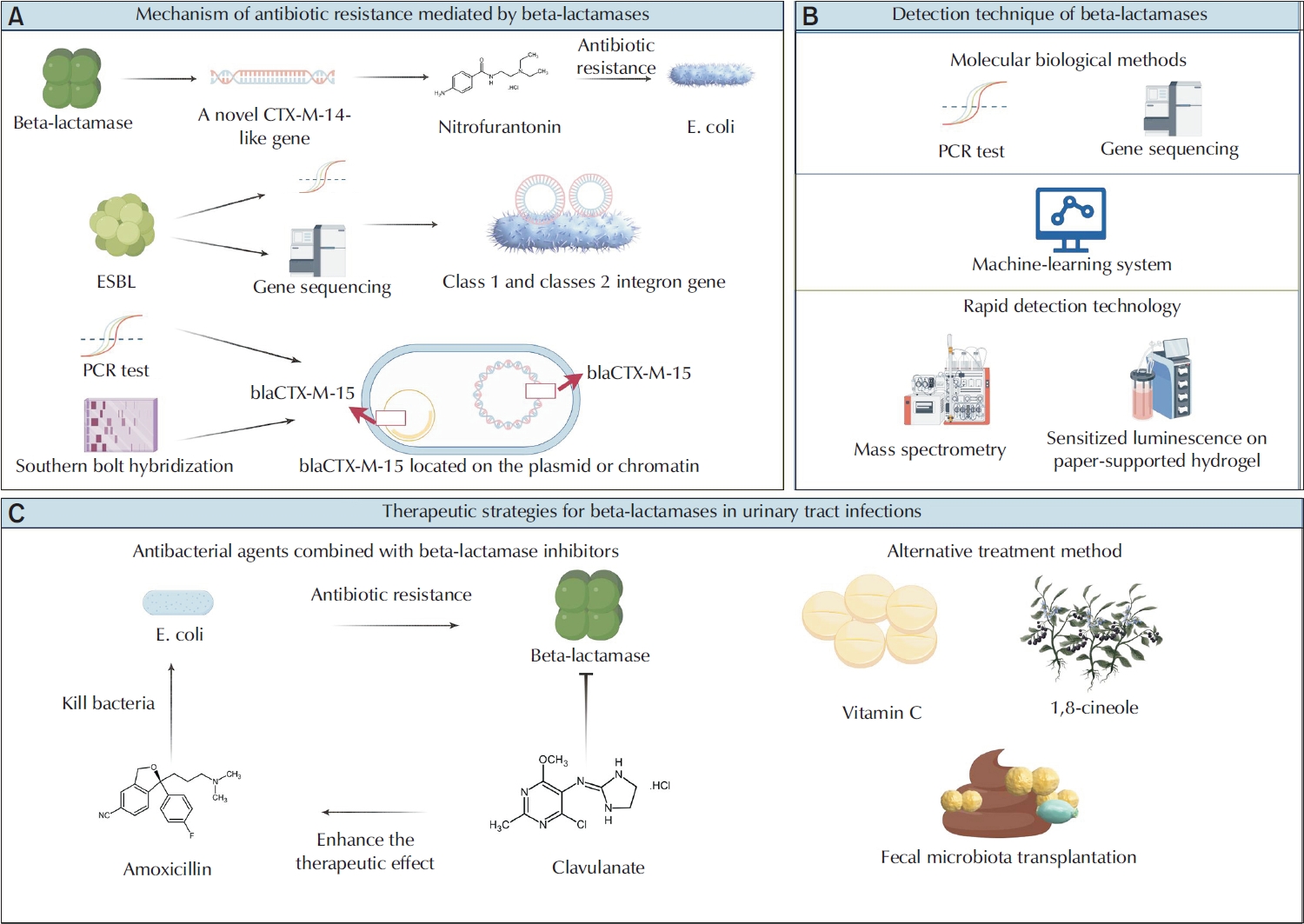
- Urinary tract infections (UTIs) are among the most prevalent bacterial infections globally, and are primarily caused by Escherichia and Klebsiella. The overprescription and inappropriate use of antibiotics have accelerated the emergence of multidrug-resistant bacteria. Beta-lactamases play a critical role in mediating antibiotic resistance in UTIs. These enzymes promote bacterial resistance through multiple mechanisms, including gene mutation, plasmid-mediated horizontal gene transfer, and the involvement of integrons. Comprehensive knowledge of the ways in which beta-lactamases contribute to resistance in UTIs is essential for improving treatment strategies. Advances in detection technologies, such as gene sequencing and mass spectrometry, have greatly enhanced the ability to monitor and predict bacterial resistance. Current therapeutic strategies include the application of beta-lactamase inhibitors, the development of novel antibiotics, and alternative treatments that have shown efficacy against beta-lactamase-mediated antibiotic resistance. This paper reviews the mechanisms of beta-lactamase-mediated resistance in UTIs and provides an in-depth overview of several detection methods and therapeutic approaches.
-
Citations
Citations to this article as recorded by- Erosion of empirical therapy: a multi-regional cross-sectional study of antimicrobial resistance in community-acquired urinary tract infections in Lebanon
Soumaya Hijazi, Souraya Domiati, Kamar Al Halabi, Zeina Ayash, Mira El Charif, Bahia Maatouk, Deema Rahme
International Journal of Infectious Diseases.2026; 170: 108828. CrossRef - Editorial for Urogenital Tract Infection (UTI) 2025 Vol. 20 No. 2 – Highlights of This Issue’s Papers and the UTI Editors’ Pick
Koo Han Yoo
Urogenital Tract Infection.2025; 20(2): 55. CrossRef
- Erosion of empirical therapy: a multi-regional cross-sectional study of antimicrobial resistance in community-acquired urinary tract infections in Lebanon
- 12,618 View
- 127 Download
- 2 Crossref
Original Articles
- Impact of Antibiotics on the Efficacy of Immune Checkpoint Inhibitors in Metastatic Urothelial Carcinoma
- Do Gyeong Lim, Ho Yeon Lee, Ho Seok Chung, Eu Chang Hwang, Seung Il Jung, Dong Deuk Kwon
- Urogenit Tract Infect 2023;18(3):75-81. Published online December 31, 2023
- DOI: https://doi.org/10.14777/uti.2023.18.3.75
-
Abstract
PDFPubReader
 ePub
ePub - Purpose: Emerging evidence has suggested that prior or concurrent antibiotic (ATB) use may be associated with a poor response to immune checkpoint inhibitors (ICIs) in patients with some solid tumors. This study examined the effects of ATB use on the oncological outcomes of patients receiving ICIs for mUC.
Materials and Methods: Patients receiving ICIs for mUC between 2018 and 2020 were assessed retrospectively. Those with over three cycles of atezolizumab or pembrolizumab were included. ATB use, defined as ≥ three days within 60 days before or three months after ICI administration, was compared between groups for oncological outcomes.
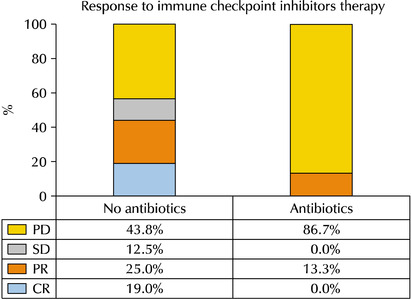
Results: Thirty-one patients were examined. The ATB-use and no-ATB-use groups consisted of 15 (48.4%) and 16 patients (51.6%), respectively. The ATB-use group showed a lower disease control rate (56.3% vs. 13.3%, p=0.023) than the no-ATB-use group. The objective response rate in the ATB-use group was lower than the no-ATB-use group, but the difference was statistically insignificant (43.7% vs. 13.3%, p=0.113). The ATB-use group had shorter progression-free survival (median three vs. six months, log-rank p=0.045) and shorter overall survival (median three vs. 14 months, log-rank p=0.023) than the no-ATB-use group. The most commonly used antibiotics were fluoroquinolones (46.7%), cephalosporins (40.0%), non-cephalosporin beta-lactams (6.7%), and nitrofurantoin (6.7%).
Conclusions: ATB may be associated with poorer oncological outcomes in patients with mUC who received ICI therapy. Hence, further research will be needed to understand the relationship between the modulation of ATB-related dysbiosis and gut microbiota composition with the oncological outcomes in patients with mUC.
- 4,437 View
- 18 Download
- Fournier’s Gangrene: A 10-Year Clinical Experience at a Tertiary Academic Medical Center
- Woo Seop Seong, Byeong Jin Kang, A Reum Kim, Kyung Hwan Kim, Hong Koo Ha
- Urogenit Tract Infect 2023;18(2):64-69. Published online August 31, 2023
- DOI: https://doi.org/10.14777/uti.2023.18.2.64
-
Abstract
PDFPubReaderePub
- Purpose: This retrospective study examined the factors influencing clinical outcomes and mortality in patients with Fournier's Gangrene (FG). The medical history, diagnostic procedures, treatment approaches, complications, and mortality factors associated with FG were analyzed.
Materials and Methods: This study retrospectively analyzed the medical records of 40 patients with FG treated over 10 years. The collected data included the patient demographics, comorbidities, vital signs, laboratory tests, Fournier’s Gangrene Severity Index (FGSI) scores, wound swab culture results, treatment approaches, and length of hospitalization.
Results: Among the patients with FG, diabetes mellitus and hypertension were the most common comorbidities. The hemodialysis dependence has been identified as a significant risk factor of mortality. In addition, septic shock and an FGSI >9 were associated with increased mortality. Escherichia coli was the most prevalent bacterium in wound swab cultures, and the presence of antibiotic-resistant bacteria was significantly higher in the non-survivors. Treatment involved broad-spectrum antibiotics, emergency surgical debridement, and subsequent adjustments based on culture results.
Conclusions: Early diagnosis and prompt initiation of treatment are essential for improving the outcomes of patients with FG. Hemodialysis dependency, septic shock, FGSI scores, and the presence of antibiotic-resistant bacteria are important factors associated with mortality in patients with FG. Further research will be needed to validate these findings and explore adjunctive therapies to enhance the patient outcomes and improve FG management. -
Citations
Citations to this article as recorded by- Computed Tomography-Based Artificial Intelligence Analysis of Myosteatosis and Its Effect on Survival in Fournier Gangrene
Byeong Jin Kang, Changmin Park, Hyun Jun Park
The World Journal of Men's Health.2026;[Epub] CrossRef - Prognostic factors and clinical outcomes in Fournier’s Gangrene: a retrospective study of 35 patients
Han Bee Hong, Jeong Woo Lee, Chan Hee Park
BMC Infectious Diseases.2024;[Epub] CrossRef
- Computed Tomography-Based Artificial Intelligence Analysis of Myosteatosis and Its Effect on Survival in Fournier Gangrene
- 5,076 View
- 22 Download
- 2 Crossref
- Korean Multicenter Study of Infectious Complications after Transurethral Prostate Surgery in Patients with Preoperative Sterile Urine
- Seong Hyeon Yu, Seung Il Jung, Eu Chang Hwang, Tae-Hyoung Kim, Jae Duck Choi, Koo Han Yoo, Jeong Woo Lee, Dong Hoon Koh, Sangrak Bae, Seung Ok Yang, Joongwon Choi, Seung Ki Min, Hoon Choi
- Urogenit Tract Infect 2022;17(3):81-88. Published online December 31, 2022
- DOI: https://doi.org/10.14777/uti.2022.17.3.81
-
Abstract
PDFPubReaderePub
- Purpose: To evaluate the efficacy of antibiotic prophylaxis and determine the risk factors of infectious complications after transurethral surgery of the prostate.
Materials and Methods: Seven hundred and seventy-two patients who underwent transurethral resection of the prostate (TURP) or holmium laser enucleation of the prostate (HOLEP) were reviewed. Of these, this study enrolled 643 patients without bacteriuria who had not received antibiotics for urinary tract infections for two weeks before surgery. The patients were divided into two groups according to the duration of the antibiotics (Group 1: less than one day, n=396 vs. Group 2: more than one day, n=247).
Results: The overall incidence of postoperative infectious complications in 643 patients was 5.0% (32/643). When postoperative infectious complications were compared according to the duration of the antibiotics (Group 1 vs. Group 2), the infectious complications rates were 5.6% (22/396) vs. 4.0% (10/247), respectively (p=0.393). When postoperative infectious complications were compared according to the duration of antibiotics (Group 1 vs. Group 2) in the TURP and HOLEP groups, the infectious complications rates were 6.3% (12/192) vs. 1.0% (1/103) (p=0.035) and 4.9% (10/203) vs. 6.0% (8/134) (p=0.677), respectively. The duration of Foley catheterization was independently associated with infectious complications (p=0.003).
Conclusions: The results showed that prolonged postoperative catheterization affects postoperative infectious complications associated with transurethral prostate surgery. Although antibiotics administered for less than one day are effective for antibiotic prophylaxis of transurethral prostate surgery, a longer antibiotic therapy is recommended for TURP. -
Citations
Citations to this article as recorded by- Evaluation of Postoperative Urinary Tract Infection and Sepsis Rates After Adding Cystolitholapaxy to HoLEP:
A Retrospective Analysis
Federico Rovegno, Rajiv Pillai, Zafar Maan, Soumendra Datta, Omar Nasir, Gerald Rix
International Journal of Clinical Urology.2026; 10(1): 1. CrossRef
- Evaluation of Postoperative Urinary Tract Infection and Sepsis Rates After Adding Cystolitholapaxy to HoLEP:
A Retrospective Analysis
- 6,367 View
- 40 Download
- 1 Crossref
 First
First Prev
Prev

