Cyclic Hematuria Misdiagnosed as Hemorrhagic Cystitis in a Rare Case of Vesicouterine Fistula Post-Cesarean Section: A Case Report of Youssef Syndrome
Article information

Abstract
Vesicouterine fistulas are rare complications that may occur following cesarean sections and are frequently misdiagnosed due to their diverse clinical presentations. This report presents a case involving a small vesicouterine fistula initially managed conservatively, which later manifested as cyclic hematuria mimicking hemorrhagic cystitis, ultimately leading to a diagnosis of Youssef syndrome. A 45-year-old woman developed persistent vaginal urinary leakage 3 weeks after a cesarean section. Diagnostic evaluation confirmed a small (<1 cm) vesicouterine fistula. Conservative management with Foley catheterization resulted in spontaneous closure. Four months later, the patient experienced cyclic gross hematuria and dysuria without menstruation, and was subsequently diagnosed with Youssef syndrome. Hormonal therapy using continuous oral contraceptives successfully resolved the hematuria, providing a noninvasive therapeutic option. This case highlights the importance of considering Youssef syndrome in patients with cyclic hematuria after cesarean section, in order to distinguish it from hemorrhagic cystitis and ensure timely, appropriate management.
HIGHLIGHTS
This report details a rare case of a vesicouterine fistula post-cesarean section that manifested as Youssef syndrome after spontaneous closure following conservative management. The patient's cyclic hematuria mimicked hemorrhagic cystitis, underscoring the need for accurate diagnosis. Hormonal therapy with continuous oral contraceptives was a successful noninvasive treatment, highlighting an effective management option for this unusual condition.
INTRODUCTION
Vesicouterine fistulas, rare complications of obstetric procedures like cesarean sections, account for 1%–4% of all urogenital fistulas, with an estimated incidence of 0.01%–0.1% post-cesarean [1]. Youssef syndrome, characterized by cyclic hematuria (menouria), amenorrhea, and a fistulous connection between the bladder and uterus, poses significant diagnostic challenges due to its rarity and variable presentation, often mimicking conditions like hemorrhagic cystitis [2]. Delayed symptom onset, as seen in this case, further complicates diagnosis, as initial fistula closure may mask persistent endometrial communication. This case report describes a vesicouterine fistula initially managed conservatively, later presenting as Youssef syndrome, highlighting the need for heightened clinical suspicion to avoid misdiagnosis and ensure appropriate management.
CASE REPORT
A 45-year-old female (gravity 3, parity 3) with no significant medical history, presented 3 weeks post-cesarean section with continuous vaginal urinary leakage. Physical examination revealed no vaginal bleeding or hematuria, but leakage suggested a postoperative fistula. Cystoscopy identified a 0.5- to 1-cm fistula on the posterior bladder wall (Fig. 1A), confirmed by computed tomography demonstrating contrast within the uterine cavity (Fig. 1B). Conservative management with a Foley catheter for six weeks was initiated due to the small fistula size. Postcatheter removal, cystoscopy and an indigo carmine test confirmed no leakage, indicating spontaneous closure. Four months later, the patient reported gross hematuria and dysuria without vaginal leakage. Suspecting hemorrhagic cystitis, empirical antibiotic therapy (ciprofloxacin 500 mg twice daily for 7 days) was initiated, temporarily resolving symptoms. However, cyclic hematuria recurred monthly for 3 cycles, lasting 3–5 days, replacing menstruation. Urine analysis during each episode of hematuria revealed gross hematuria with many red blood cells and some pyuria, with no bacteria identified on urine culture. Bladder ultrasound revealed a persistent defect at the fistula site with uterine mucosal adherence (Fig. 1C). Youssef syndrome was diagnosed based on cyclic hematuria, amenorrhea, and imaging evidence of endometrial-bladder communication [3]. As the patient had no desire for future pregnancies, she opted for hormonal therapy with continuous combined oral contraceptives (levonorgestrel/ethinyl estradiol) to induce amenorrhea. After 3 months of therapy, hematuria resolved, with no recurrence at 6-month follow-up.
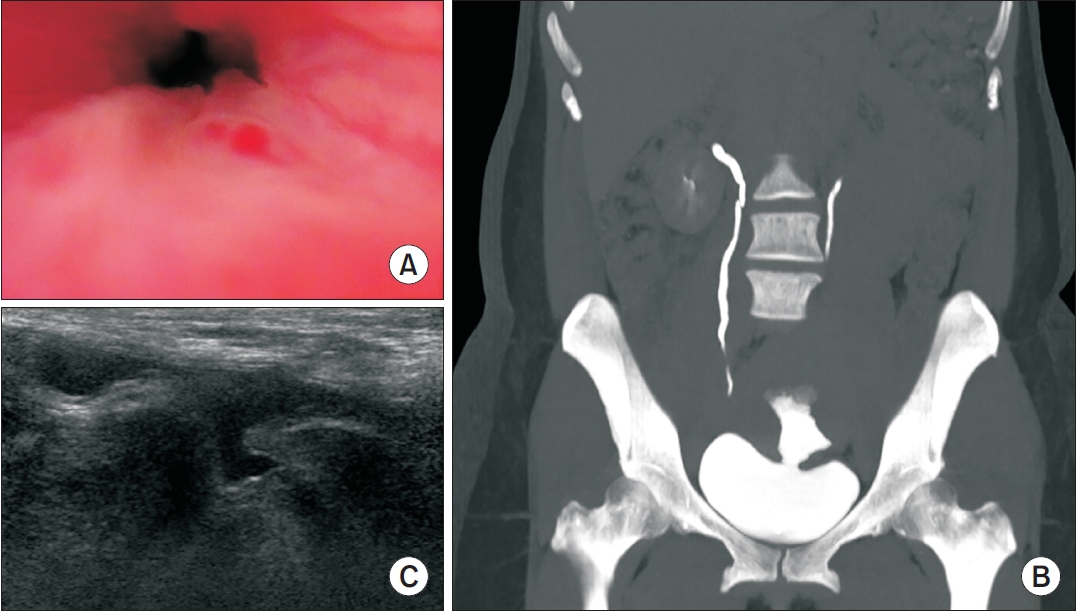
(A) Cystoscopy identified a 0.5- to 1-cm fistula on the posterior bladder wall. (B) Computed tomography demonstrating contrast within the uterine cavity. (C) Ultrasound revealed a persistent defect at the site of the previous vesicouterine fistula, with adherence to the uterine mucosa.
DISCUSSION
This case highlights a vesicouterine fistula post-cesarean section, initially resolved through conservative management, which later presented with cyclic hematuria misdiagnosed as recurrent hemorrhagic cystitis. Small vesicouterine fistulas (<1 cm) may close spontaneously with prolonged bladder catheterization within 6–12 weeks. The patient’s subsequent presentation with monthly hematuria in the absence of vaginal menstruation strongly suggested Youssef syndrome, characterized by menouria due to retrograde menstrual flow through a vesicouterine fistula. Unlike typical vesicouterine fistulas, which often present with persistent urinary leakage, this patient’s fistula appeared to have closed. However, the recurrence of cyclic hematuria indicated residual endometrial communication with the bladder [4]. This phenomenon distinguishes Youssef syndrome from common urogenital infections, such as hemorrhagic cystitis. While hormonal therapy, as chosen here, effectively suppresses menstruation, reducing menouria, with success rates of 60%–70% in non-surgical candidates [5], this patient opted for hormonal suppression as a noninvasive approach. The protrusion of uterine endometrial mucosa and cervical fibrosis contribute to maintaining continence by obstructing the fistulous opening and internal uterine orifice, respectively, redirecting menstrual flow into the bladder. The absence of urinary incontinence can be explained by pressure gradients between the uterus and bladder. Bladder pressures remain relatively low during filling (5–20 cmH2O) and voiding (30–50 cmH2O), while intrauterine pressures fluctuate significantly, reaching 130 –160 cmH2O during menstruation and 35–100 cmH2O during the intermenstrual phase (Fig. 2). These elevated uterine pressures ensure that uterine contents preferentially flow into the bladder, preventing urinary leakage into the vagina [6]. Long-term follow-up is essential to monitor recurrence, particularly in conservatively managed cases.
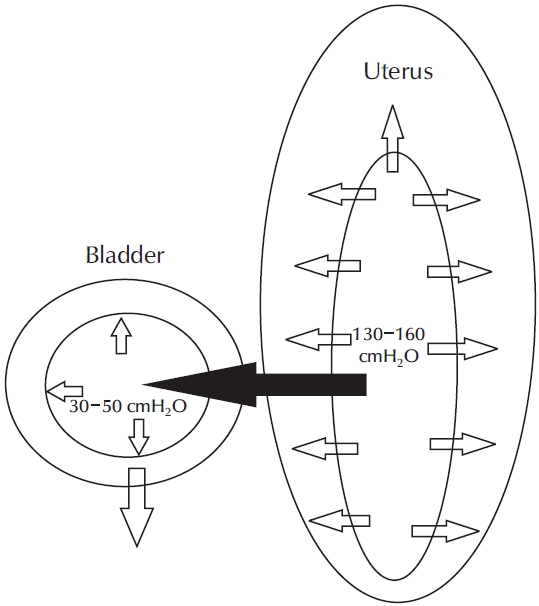
The pressure gradient between the uterus and bladder drives menstrual flow into the bladder in Youssef syndrome. During menstruation, intrauterine pressures reach 130–160 cmH₂O due to uterine contractions, significantly exceeding bladder pressures of 5–20 cmH₂O (filling) and 30–50 cmH₂O (voiding). In the intermenstrual phase, intrauterine pressures of 35–100 cmH₂O remain higher than bladder pressures, preventing urinary leakage into the vagina. Cervical fibrosis and mucosal adherence at the fistula site further impede retrograde urinary flow, explaining the absence of incontinence while allowing menouria.
This report's strength is its detailed documentation of a rare, delayed presentation of Youssef syndrome. However, its limitations include the lack of generalizability inherent to a single case study and the absence of definitive histological confirmation, as the patient opted for non-surgical management.
Notes
Funding/Support
This work was supported by the 2025 education, research, and student guidance grant funded by Jeju National University.
Research Ethics
This study was approved by the Institutional Review Board (IRB) of School of Medicine, Jeju National University (IRB No. JEJUNUH 2025-02-013). Written informed consent by the patient was waived by the IRB due to a retrospective nature of our study.
Conflict of Interest
The authors have nothing to disclose.
Author Contribution
YJK is the single author of this study.