Giant Fibroepithelial Polyp in the Renal Pelvis to the Upper Ureter
Article information

Abstract
Benign ureteral tumors are rare owing to the predominance of malignancies in ureter tumors. Among them, fibroepithelial polyps are very rare, and giant fibroepithelial polyps are even rarer. This paper reports the author’s experience of giant fibroepithelial polyps detected incidentally. A 47-year-old woman was referred for severe right flank pain to the author’s center. A kidney computed tomogram revealed a long soft tissue lesion in the right kidney, upper polar calyx, pelvis, and whole proximal ureter with hydronephrosis. The radiologic reading was right renal pelvis urothelial cancer. Endoscopic removal was deemed impossible because the mass was filling the entire renal pelvis and upper ureter, so a nephroureterectomy was performed. After the nephroureterectomy, the pathology findings revealed a giant fibroepithelial polyp. This paper reports the treatment of giant fibroepithelial polyps of the ureter. Clinicians should consider the possibility of benign tumors and recommend a cautious approach to treatment if discovered.
Fibroepithelial polyps are rare benign tumors of the ureter with a mesodermal origin. A 47-year-old woman was referred to our center for severe right flank pain. Appropriated treatment of fibroepithelial polyp might be renal saving surgery like ureterectomy with ene-to-end anastomosis or ureteroscopic polypectomy. However, in our case, large mass filled out from calyx to proximal ureter and the patient underwent nephroureterectomy for possible transitional cell carcinoma.
CASE REPORT
A 47-year-old woman presented to the author’s depart-ment with severe right flank pain without fever or hematuria. She had no risk factors for acute pyelonephritis and showed stable vital signs, including body temperature. The physical examination showed no remarkable findings, but she complained of severe costovertebral angle tenderness. The patient had no significant past disease history, including ureter stones, tuberculosis, and malignant tumors, and there was no significant family history. There was no abnormality in complete blood count and serum chemical analysis, including the blood urea nitrogen/Creatinine level. Initial urine analysis showed normal findings except more than 100 red blood cells per high-powered field. Urine cytology detected no abnormal cells.
A kidney computed tomogram (CT) was recommended for work-up, which revealed a soft tissue filling defect from the upper calyx of the right kidney and full pelvis to the upper ureter approximately 10 cm in length. The radiology reading indicated renal pelvis urothelial cancer (Fig. 1). CT and bone scan showed no evidence of lymph node invasion or distant metastasis. The risk of malignancy was estimated to be very high statistically. Based on the CT findings, a complete ureteroscopic resection of the tumor would be very difficult considering the size and the position that filled the ureter and pelvis, even if it were not a cancer. Therefore, a decision was made to perform a nephroureterectomy.
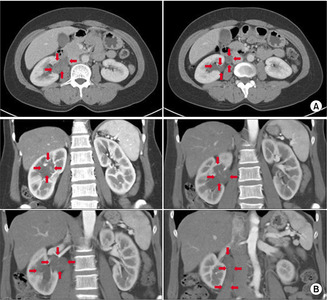
(A) Computed tomography axial view, (B) computed tomography coronal view. The red arrows indicate tumor extent.
A hand-assisted laparoscopic nephroureterectomy was performed. Bladder cuffing was not performed because the frozen biopsy performed during surgery revealed the tissue to be benign fibrosis. The tumor was a round, long, and easily distinguishable soft mass with good demarcation compatible with the expression of a worm-like projection starting from a renal upper-portion calyx (Fig. 2). The patient recovered well without complications, such as bleeding or infection, and was discharged seven days after surgery.
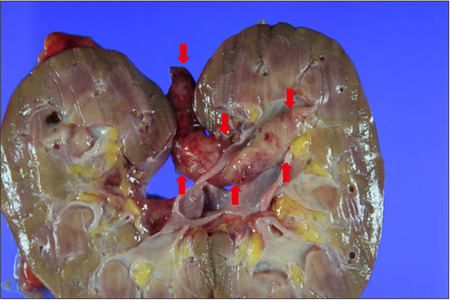
Gross section: red arrows indicate tumor extent. The base of the polyp originated from the upper calyx and attached segment of the tumor measuring 8.5×2.0×1.4 cm in size. The external surface was smooth and gelatin-like, and the polypoid mass. The red arrows indicate a tumor.
The fibroepithelial polyp was finally diagnosed as a well-demarcated tumor from the pathology reports. The base of the polyp originated from the upper calyx, and the attached segment of the tumor measured 8.5×2.0×1.4 cm in size. The external surface was smooth and gelatin-like, and the polypoid mass was covered with a normal urothelial cell layer and loose fibrous and inflammatory tissue (Fig. 3). No demonstratable atypical cells were observed in the specimen. The patient has been doing well with no signs of recurrence over the subsequent four-year follow-up. Authors received informed consent for the use of the patients’ photographs or other information through the publication.
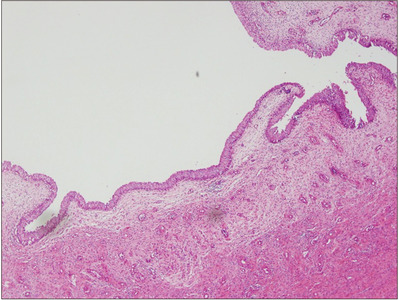
Microscopic section: the polypoid mass was covered with a normal urothelial cell layer and loose fibrous and inflammatory tissue (H&E, ×40).
DISCUSSION
Fibroepithelial polyps are rare benign tumors of the ureter with a mesodermal origin in the same category as leiomyoma, fibroma, neurofibroma, and lymphangioma [1]. Unlike a transitional cell carcinoma or squamous cell carcinoma derived from the epithelium, it was differentiated from mesenchymal tissue [2]. The most common symptoms are hematuria for necrotic changes and intermittent flank pain for long periods [3,4]. Both congenital and acquired factors are assumed to be the cause of origin, e.g., hormonal imbalance, allergic reaction, infection, chronic inflamma-tion, and ureteral obstruction. On the other hand, the exact pathogen was not identified [5,6]. The condition is more common in males and on the left side [7]. Most cases (approximately 84.4%) are single tumors, but up to 15.2% of tumors are on the bilateral sides, and the size of the tumor is approximately 4.0 cm (0.4-17.0 cm) [8]. Fibroepithelial polyps are observed in any part of the ureter, but the upper ureter, including the ureteropelvic junction, is the most common (63%), and polyps of the renal pelvis or calyx are rare [8].
There are few reports on the radiology findings of fibroepithelial polyps. Intravenous urography typically reveals a round, polypoid filling defect surrounded by a contrast material-shaped corkscrew, finger, or worm-like projection [9,10]. A continuous rim of contrast media surrounding the central part and tumor attached to the ureter wall was observed by CT [11]. Renal function deterioration is very rare, but long-standing back pressure caused by complete obstruction has been suggested to lead to cortical atrophy. In the present patient, the hydronephrosis was not as severe. Generally, in the case of ureteral tumors, a treatment modality is determined after disease confirmation through ureteroscopic biopsy. In the case of benign tumors, appropriate treatment might be renal-saving surgery like ureterectomy with end-to-end anastomosis or ureteroscopic polypectomy.
In the present case, however, the patient underwent a nephroureterectomy without a ureteroscopic biopsy, and there may be controversy in this regard. Initially, a ureteroscopic biopsy was considered, but the possibility of it being benign was statistically low, and the actual tumor was so large and extensive that it filled the calyx, pelvis, and upper ureter, so it was decided to be even less likely. Moreover, it was thought that a clean and complete resection of the tumor endoscopically would be complicated. Hence, a nephroureterectomy was ultimately considered the most efficient treatment without a ureteroscope biopsy. Although it is gradually decreasing, the reason why nephroureterec-tomy is still performed in approximately 8.8% of cases in a systemic review is probably due to a similar reason [8]. Therefore, the higher and larger the tumor is, the higher the probability of surgical removal. In this way, when making clinical decisions, there are cases where surgical removal is judged to be in the best interest of the patient, even if not in principle. On the other hand, although the probability was low, it is in the patient’s long-term interests to be aware of the possibility of a benign tumor and the possibility of success with a less invasive treatment. Hence, more active and diverse attempts should be considered.
The recurrence of fibroepithelial polyps is extremely rare, and no recurrence has been reported in 108 cases in which a resection had been performed. No recurrence was reported in 108 cases who underwent open incision surgery, 10 cases of ureteroscopic laser ablation, and one case of transurethral resection surgery [6,12].
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING
No funding to declare.