Spontaneous Bladder Perforation in a Patient with a Long-Term Intraurethral Catheter
Article information

Abstract
Urinary catheters are commonly used to address various urinary problems. However, the catheter itself can be a cause of several complications, including catheter-associated urinary tract infections, damage to the bladder and kidneys, and, in extremely rare cases, bladder perforation. We present a case of spontaneous bladder perforation in a patient who had a long-term indwelling intraurethral catheter. The patient with prior hypoxic brain damage suddenly developed tachypnea, tachycardia, and oxygen desaturation. Computed tomography and retrograde cystography revealed an extraperitoneal bladder perforation with an intra-pelvic abscess. Antibiotics were prescribed and a urinary catheter was inserted for drainage. After 11 weeks, the abscess resolved, and the catheter was removed to enable self-voiding. The perforation was attributed to chronic inflammation and distension of the bladder wall caused by the intraurethral catheter. Given the potential complications associated with long-term urinary catheterization, the timely removal of indwelling catheters should be considered.
Bladder perforation is a relatively rare condition and is caused by blunt abdominal trauma and iatrogenic injury to the pelvis during endoscopic interventions or surgery. Spontaneous bladder perforation is an even less common, but life-threatening event induced by chronic inflammation, bladder outflow obstruction, or cancer [1]. Symptoms of bladder perforation include lower abdominal pain, dysuria, anuria, and hematuria. An intraperitoneal perforation can show signs of peritonitis. Taking a thorough history and physical examination are important for diagnosis and management. Radiographic evaluation, including retrograde cystography and computed tomography (CT), helps confirm the diagnosis and assess complications. A bladder perforation can be either intra- or extraperitoneal [2-4]. An extraperitoneal perforation without any complications can be managed non-operatively by placing an indwelling intraurethral catheter, but an intraperitoneal perforation may require surgical repair. In this report, we present a case of spontaneous bladder perforation in a patient with a long-term indwelling urinary catheter. Institutional Review Board of Kwangju Christian Hospital approved exemption for review as the study was retrospective case report.
CASE REPORT
1. Clinical Presentation
A 78-year-old female was found unconscious, jammed between farm machinery and a tree. She had suffered a cardiac arrest but was successfully resuscitated. Initial evaluation revealed bilateral hypoxic brain damage, multiple rib fractures, pulmonary hemorrhage in both lungs and edematous changes in the gall bladder and colon. She was transferred to our facility soon after acute management. She had a comatose mental status; a tracheostomy tube, an intraurethral catheter, and a nasogastric tube were inserted. Comprehensive rehabilitation was done, including passive range-of-motion exercises, to prevent joint contracture. A month after admission, her urine became turbid with a large amount of mucosal plug, which led to frequent catheter obstruction and peri-catheter leakage of urine. Hence, we irrigated the bladder through the catheter with normal saline daily and changed the urinary catheter at 1-2-week intervals. Two months after admission, the patient suddenly developed tachypnea, tachycardia, and oxygen desaturation. Hema-turia, pyuria, and a large amount of sputum were also noted. Her vital signs and lab data were as follows: respiratory rate 22 breaths/min, pulse 150 beats/min, blood pressure 150/90 mm Hg, and peripheral oxygen saturation level 85%. Her C-reactive protein and d-dimer levels were elevated. We transferred her to the intensive care unit. Initial evaluation with an enhanced chest CT revealed bilateral lower lobe consolidation suggesting pneumonia and a thromboembo-lism in the left pulmonary artery. A few hours later, she showed signs of septic shock. Her blood pressure was 80/50 mm Hg, she had a fever of over 38°C, and her total urine output was only 600 ml/24 hours despite an input of 1,800 ml/24 hours. The pneumonia did not appear sufficiently severe to cause septic shock. Abdominal and pelvic CT (APCT) revealed fluid collection and focal free air in the pelvis, which suggested the possibility of extraperitoneal abscess formation. Immediate retrograde cystography revealed the leakage of contrast material through the anterolateral bladder wall (Fig. 1). Authors received informed consent for the use of the patients’ photographs or other information through the publication.
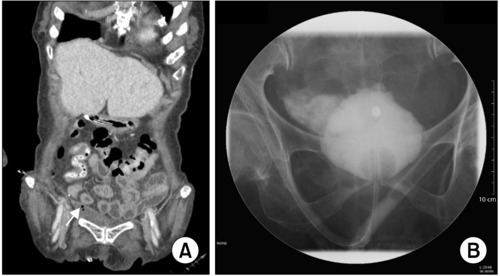
(A) A computed tomography scan showing extraperitoneal free air and fluid collection suggestive of an abscess (arrow: free air). (B) Cystography showing leakage of the contrast material outside the bladder wall.
2. Management
As the case comprised extraperitoneal bladder perforation with an intrapelvic abscess formation, surgical treatments might have been the best choice. However, the patient was non-operable due to concomitant medical conditions. Conservative treatments with urethral catheter drainage and antibiotics were chosen. Since the abscess was small and her immediate familiy did not want an invasive procedure, percutaneous drainage was not performed. Instead, the urinary catheter was changed to one of a smaller diameter to minimize further bladder insult and to drain urine. Continuous bladder irrigation with sterile saline was done to prevent outflow obstruction. Also, we changed the antibiotics according to the results of the culture test (Table 1). Since extended-spectrum beta-lactamase positive Klebsiella pneumoniae was identified in the first urine culture test, meropenem was administered. Subsequently, the patient tested positive for multidrug-resistant Acineto-bacter baumannii in the sputum culture, and the antibiotic was replaced with colismethate. After treatment with the antibiotic for two weeks, the patient was maintained on piperacillin/tazobactam treatment until the abscess completely disappeared on the CT. Cystography performed 2 weeks later revealed no leakage from the bladder wall (Fig. 2). As cystography itself can stress the wall, we decided not to repeat the examination. Rather, we performed a CT at 1-month intervals.

Progression notes of the patient showing antibiotics used, abscess diameter in CT, CRP levels
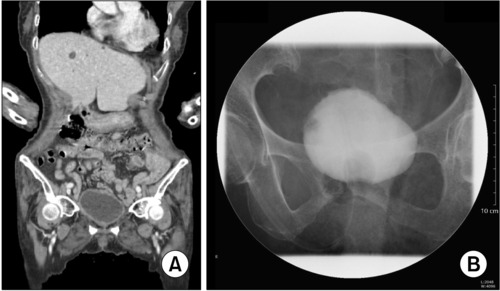
(A) A computed tomography scan showing that the abscess has resolved. (B) Cystography reveals no contrast leakage.
3. Outcome
The patient was maintained on antibiotics for 11 weeks (Table 1). CT was last performed in October 2021, which confirmed the resolution of the intra-pelvic abscess (Fig. 2). A few weeks later, the indwelling catheter was removed, and the patient was able to self-void successfully; the post-voiding residual volume was below 50 ml and the voiding frequency of 200-300 ml/3-4 hours was acceptable. She was free from any bladder complications but passed away due to an acute exacerbation of pneumonia four months later.
DISCUSSION
Spontaneous bladder perforation is very rare, but it is a life-threatening event. Therefore, prompt diagnosis and appropriate management are important. It was challenging for us to establish a proper diagnosis due to the presence of concomitant medical conditions and the patient’s inability to communicate her subjective symptoms. We had to rely on physical examination, vital signs, and laboratory data to arrive at an initial impression. Key signs that suggested bladder perforation included a sudden decrease in urine output, hematuria, and pyuria. The fact that the pneumonia was not severe enough to cause septic shock led us to consider other causes. Hence, we performed APCT and retrograde cystography. The imaging studies revealed extraperitoneal bladder perforation.
According to the guidelines of the American Urology Association, uncomplicated extraperitoneal bladder injuries can be managed conservatively with a urethral catheter, but complicated ones may require surgical repair. Intrapelvic abscess formation was seen in our patient with signs of septic shock, which is indicative of a complicated injury. Conservative management includes extravesical drainage, which is performed in about 1.5% of extraperi-toneal bladder perforation during transurethral resection [5]. The authors couldn’t find any consensus for extravesical drainage of the pelvic abscess due to bladder perforation, but in a study by Dick et al. [6] it has been suggested that it is important if the urine is infected. Thus, the application of percutaneous drainage may have helped the healing process in this case.
Multiple factors led to bladder perforation in this patient. The patient exhibited chronic pyuria, a mucosal plug in the urinary bag, and frequent leakage of urine outside the catheter. The findings suggested a catheter-associated urinary tract infection, which led to a chronic inflammation of the bladder wall and made it vulnerable to stress. In addition, the mucosal plug led to catheter obstruction and distension of the bladder wall, which is thought to be the primary cause of acute bladder perforation. Two months prior, she had experienced blunt abdominal trauma, which could have resulted in a contusion of the bladder wall. In general, bladder injury after abdominal trauma is closely related to both pelvic fracture and gross hematuria [7]. Neither was present during her initial evaluation after the accident. However, subsequent infla-mma-tion of the damaged mucosal and muscular layers may have contributed to the perforation. Furthermore, prior to the occurrence of bladder perforation, we conducted normal saline irrigation manually and through gravity feed due to frequent urine stream obstructions. This procedure, especially manual irrigation, which applies greater pressure to the bladder, could have placed stress on the bladder wall. According to a study conducted by Elliott et al. [8], when bladder irrigation was performed on patients with long-term intraurethral catheters or chronic urinary tract infections, there was an elevated rate of urothelial cell exfoliation compared to the control group. This essentially exacerbated the damage to the already compromised urothelium. Additionally, in a case report by Di Paolo et al. [9], urothelial disruption occurred after bladder irrigation, which led to the absorption of a massive amount of fluid through the bladder wall. In summary, chronic inflammation and distension of the bladder wall caused by the intraurethral catheter contributed to the acute perforation, which was compounded by the manual irrigation of the bladder. The traumatic wall contusion might have been related to the accident itself. Urinary catheters are frequently used to address urine retention, and incontinence due to various causes. However, they are often used only to reduce the burden of the healthcare providers rather than to relieve patient discomfort. In this case, we emphasize the potential risk of long-term indwelling urinary catheters. The daily infection rate of such catheters is about 5%; up to 95% of patients exhibit bacterial infections after one month [10]. Other possible complications of catheters include chronic infection, kidney and bladder damage, and bladder stones [10]. Bladder perforation is a rare but severe and life-threatening complication. Therefore, even if the patient is unconscious, evaluation of the bladder function is necessary, and continuous attempts to withdraw the catheter should be made.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING
No funding to declare.
AUTHOR CONTRIBUTIONS
T.C. participated in data collection and wrote the manuscript. H.L., S.L., Y.C., E.K. and J.K. provided professional opinions on the journal. J.K., S.L., E.N. contributed on data collection. All authors read and approved the final manuscript.