Stone-Free Rates of mPCNL, PCNL, and RIRS: A Systematic Review and Network Meta-Analysis
Article information

Abstract
Purpose
Retrograde intrarenal surgery (RIRS) and percutaneous nephrolithotomy (PCNL) are performed to treat renal stones, and miniature PCNL (mPCNL) is used as an alternative to conventional PCNL. We conducted a systematic review of published studies regarding RIRS, PCNL, and mPCNL and performed network meta-analysis on successful outcome (stone-free) rates.
Materials and Methods
The PubMed and EMBASE databases were searched up to December 2020. Data extraction formats were used to extract data on successful outcome rates, study designs, numbers of subjects and characteristics, and methods used to treat renal stones (i.e., RIRS, PCNL, or mPCNL).
Results
Data obtained by 25 studies were used to compare the stone-free rates of RIRS, PCNL, and mPCNL; six comparisons of PCNL and mPCNL, seven of mPCNL and RIRS, and 12 of RIRS and PCNL were analyzed. No difference was found between the stone-free rates of PCNL and mPCNL (odds ratio [OR]: 0.96; 95% confidence interval [CI]: 0.51-1.9) by network meta-analysis. However, the stone-free rate of RIRS was lower than that of mPCNL (OR: 0.41; 95% CI: 0.021-0.82) and PCNL (OR: 0.43; 95% CI: 0.22-0.82). Ranking analysis ranked mPCNL as No. 1 and PCNL as No. 2.
Conclusions
PCNL and mPCNL had better stone-free rates than RIRS for the treatment of renal stones, but the treatment outcomes of PCNL and mPCNL were no different.
INTRODUCTION
Mini-percutaneous nephrolithotomy (mPCNL) was developed to treat pediatric patients with renal stones [1]. Helal et al. [2] first performed mPCNL in 1997 in a 2-year-old pediatric patient using a 15-Fr Hickman peel-away sheath. Currently, mPCNL is defined as PCNL performed using access sheaths of diameter 14-20 Fr [3] and has advantages over standard PCNL in terms of blood loss, postoperative pain, and renal parenchymal damage, which are complications associated with the larger instruments used for standard PCNL [4]. However, despite these advantages, mPCNL is not considered the preferred technique [5,6].
The European Association of Urology (EAU) Urolithiasis Guidelines state that mPCNL requires a longer operating time and recommend that additional studies be conducted to determine treatment outcomes [7]. Furthermore, these guidelines recommend extracorporeal shock wave lithotripsy (ESWL) and retrograde intrarenal surgery (RIRS) as first-line treatments for kidney stones <2 cm in diameter, and that PCNL be considered the first-line treatment for stones >2 cm [7]. For lower pole stones of 1-2 cm, endourologic procedures, including RIRS and PCNL, are recommended for patients with unfavorable factors for ESWL, which is the only non-invasive interventional treatment and plays a pivotal role in the treatment of urinary stones [8,9]. On the other hand, RIRS has the advantage of being less invasive than PCNL and mPCNL due to the use of a natural orifice [10]. PCNL remains the standard treatment for renal stones >2 cm and is considered the first treatment option for large stones resistant to shock waves [11]. mPCNL has fewer complications than PCNL when performed in selective patients [12]. Prospective studies and meta-analyses have compared PCNL, mPCNL, and RIRS and discussed their advantages and disadvantages. Network meta-analysis is a research method that enables direct and indirect comparisons of multiple treatments [13-15], but no network meta-analysis has been conducted to compare the outcomes of these three modalities simultaneously. Accordingly, we performed a systematic review and utilized network meta-analysis to compare the stone-free rates of PCNL, mPCNL, and RIRS.
MATERIALS AND METHODS
1. Inclusion Criteria
Publicly available randomized controlled trials that met the following criteria were included: (1) Evaluation of 2 or 3 arms, including PCNL, mPCNL, and RIRS for the treatment of kidney stones; (2) Baseline data on matched 2 or 3 patient groups, including the number of patients included and values of indices; (3) The use of stone-free rates to analyze treatment results; (4) The use of standard surgical indications for each treatment; (5) The inclusion of complication rates among endpoint outcomes; and (6) Publication in the English-lan-guage. This study was performed using the Preferred Reporting Item for System Review and Meta-Analysis (PRISMA) guidelines (accessible at http://www.prismastatement.org/) (Supplementary Table 1) [16].
2. Search Strategy
All literature searches were conducted using the PubMed and EMBASE databases before December 31, 2020. Cross-reference searches were also conducted to identify articles missed during the computerized literature search. The progress reports of relevant meetings were also reviewed. Medical Subject Headings (MeSHs) and keywords were searched using percutaneous nephrolithotomy, nephrolithotomy, percutaneous, flexible ureteroscopy, flexible, ureterorenoscopy, retrograde intrarenal surgery, renal stone, urolithiasis, success rate, miniature, mini, and stone-free.
3. Data Extraction
One author (JYL) screened all titles and abstracts found using the literature search. Two other authors (DHK and HDJ) independently analyzed all articles in detail to ensure that they met the inclusion criteria. Disagreements between the two researchers were resolved by discussion until consensus was reached or by third-party adjudication by another author (DYC).
4. Quality Assessment of Studies
When final articles were agreed, two researchers independently examined the quality of each article using the Downs and Black checklist, which was developed for the quality assessment of randomized and non-randomized studies on health interventions [17]. The checklist consists of five subscales, viz. reporting, internal validity bias, internal validity confounding, external validity, and power. Because six items were related to intervention, randomization, and power calculation, and not all studies included were randomized studies, scores of zero were allocated to these six items, as previously suggested [18]. Therefore, the maximum possible quality score was 31 points. Higher scores indicated better study qualities.
5. Heterogeneity Tests
Heterogeneity of included studies was examined using the Q statistic and Higgins I2 statistic [19]. Higgins I2 measures the percentage of total variation due to heterogeneity rather than chance across studies and was calculated as follows:
where 'Q' is Cochran's heterogeneity statistic, and 'df' is the number of degrees of freedom.
An I2 value of ≥50% is considered to indicate substantial heterogeneity [20]. For the Q statistic, heterogeneity was deemed to be significant for p-values <0.10 [21]. When there was evidence of heterogeneity, data were analyzed using a random-effects model. Studies with confirmed positive results were assessed using pooled specificity and 95% confidence intervals (CIs). In addition, Galbraith radial and L'Abbe plots were used to evaluate heterogeneity [22,23].
6. Statistical Analysis
Outcome variables measured at specific time points were compared using odds ratios (ORs) or mean differences with 95% CIs using network meta-analysis. Analyses were based on non-informative priors for effect sizes and precision. Convergence and lack of auto-correlation were confirmed after four chains and a 50,000-simulation burn-in phase. Finally, direct probability statements were derived from an additional 100,000-simulation phase. The probabilities that each modality had the lowest rate of clinical events were assessed by Bayesian Markov Chain Monte Carlo modeling. Sensitivity analyses were performed by repeating the main computations using a fixed-effects model. Model fit was appraised by computing and comparing estimates for deviance and deviance information criteria. The statistical analysis was performed using R (R version 3.3.2; R Foundation for Statistical Computing, Vienna, Austria; http://www. r-project.org) with associated meta, netmeta, pcnetmeta, and gemtc packages for pairwise and network meta-analyses.
RESULTS
1. Eligible Studies
A total of 289 studies were originally identified. After screening, 46 articles were assessed for eligibility, and 16 of these studies were excluded for the following reasons: 6 articles did not have data on stone-free rates, 11 articles were review articles, and 4 articles were case report series. Finally, the remaining 25 studies were included in the meta-analysis (Fig. 1).
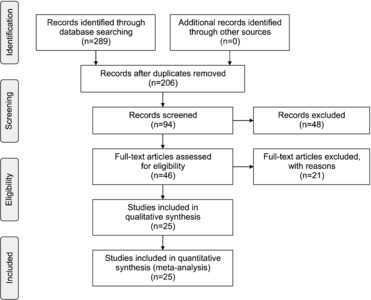
Flow diagram of evidence acquisition. Twenty-five studies were ultimately included in the qualitative and quantitative syntheses that involved pairwise and network meta-analyses.
Data associated with confounding factors derived from each study are summarized in Table 1. Eight studies compared PCNL and mPCNL [5,24-30], ten trials reported PCNL and RIRS outcomes [31-40], and seven studies compared mPCNL and RIRS outcomes [41-47] (Fig. 2). Table 1 provides a summary of the data, including stone-free rates, of the enrolled studies.

Studies included in the meta-analysis
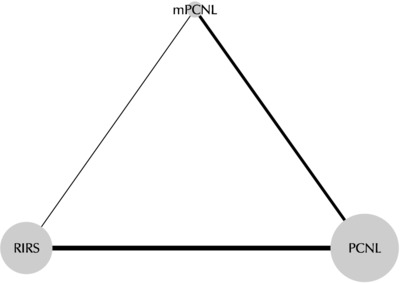
Network plots for the included studies. Eight studies compared percutaneous nephrolithotomy (PCNL) versus miniature percutaneous nephrolithotomy (mPCNL), seven trials reported the outcomes of mPCNL and retrograde intrarenal surgery (RIRS), and ten studies compared the outcomes of PCNL and RIRS.
2. Quality Assessment
The results of quality assessments based on the Downs and Black checklist are shown in Table 1. Median total quality score was 15.12. Overall, quality scores within subscales were low to moderate. In particular, external validity was unsatisfactory for PCNL, mPCNL, and RIRS comparisons found to be significantly and non-significantly different.
3. Heterogeneity and Inconsistency Assessments and Publication Bias
Forest plots of the pairwise meta-analyses of mPCNL, PCNL, and RIRS are shown in Fig. 3-5. No heterogeneity was observed between PCNL and RIRS (Fig. 3); however, heterogeneity was observed between mPCNL and PCNL (I2=51.0%, p=0.05; Fig. 4), and between mPCNL and RIRS (I2=51.0%, p=0.06; Fig. 5). Thus, the random-effects model was applied using the Mantel–Haenszel method to compare mPCNL and PCNL and mPCNL and RIRS (Fig. 4, 5). After the selection of effect models, little heterogeneity was observed in L'Abbe or radial plots (Fig. 6, 7). Inconsistency was not demonstrated by node-splitting analysis for direct, indirect, or network comparisons (Fig. 8).
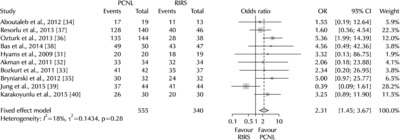
Pairwise meta-analysis of the success rates of percutaneous nephrolithotomy (PCNL) and retrograde intrarenal surgery (RIRS). Pooled data showed a significantly higher stone-free rate for PCNL than RIRS (odds ratio [OR]: 2.31; 95% confidence interval [CI]: 1.45-3.67; p<0.001).
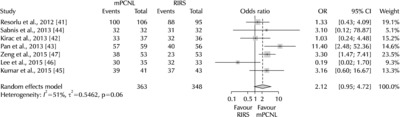
Pairwise meta-analysis of the success rates of miniature percutaneous nephrolithotomy (mPCNL) and retrograde intrarenal surgery (RIRS). The stone-free rate of mPCNL was not greater than that of RIRS (odds ratio [OR]: 2.12; 95% confidence interval [CI]: 0.95-4.72; p=0.07).
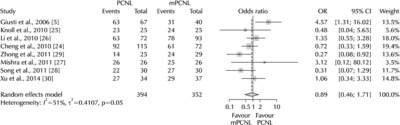
Pairwise meta-analysis of the success rates of percutaneous nephrolithotomy (PCNL) and miniature percutaneous nephrolithotomy (mPCNL). The stone-free rates of these two modalities were no different (odds ratio [OR]: 0.89; 95% confidence interval [CI]: 0.46-1.71; p=0.73).
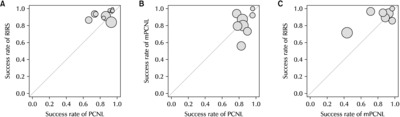
L’Abbe plots of retrograde intrarenal surgery (RIRS) and percutaneous nephrolithotomy (PCNL) (A), miniature percutaneous nephrolithotomy (mPCNL) and PCNL (B), and RIRS and mPCNL (C) success rates.
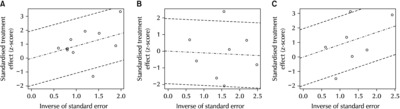
Radical plots of retrograde intrarenal surger (RIRS) and percutaneous nephrolithotomy (PCNL) (A), miniature percutaneous nephrolithotomy (mPCNL) and PCNL (B), and RIRS and mPCNL (C) success rates.
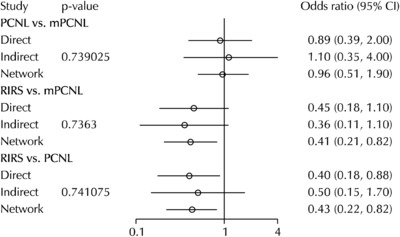
Network meta-analysis of miniature percutaneous nephro-lithotomy (mPCNL), percutaneous nephrolithotomy (PCNL), and retrograde intrarenal surgery (RIRS) success rate and node-splitting analyses of inconsistency.
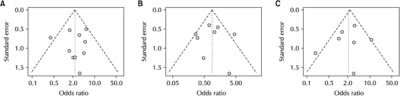
The Begg and Mazumdar rank correlation tests showed no evidence of publication bias in the present meta-analysis between PCNL and RIRS (p=0.79), PCNL and mPCNL (p=0.81), or mPCNL and RIRS (p=0.45). Similarly, Egger’s regression intercept tests showed no publication bias between PCNL and RIRS (p=0.87), PCNL and mPCNL (p=0.99), or mPCNL and RIRS (p=0.56). In addition, little evidence of publication bias was detected in funnel plots for these comparisons (Fig. 9).
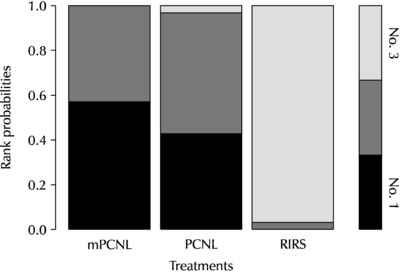
Rank-probability test of network meta-analyses. The rank-probability test ranked miniature percutaneous nephrolithotomy (mPCNL) as No. 1 and retrograde intrarenal surgery (RIRS) as No. 3. PCNL: percutaneous nephrolithotomy.
4. Pairwise Meta-Analysis of PCNL, mPCNL, and RIRS with Respect to Stone-Free Rate
Pooled data showed a significantly higher stone-free rate after PCNL (OR: 2.31; 95% CI: 1.45-3.67; p<0.001) than after RIRS (Fig. 3). No difference between stone-free rates after PCNL or mPCNL (OR: 0.89; 95% CI: 0.46-1.71; p=0.73) (Fig. 4), and a non-significantly higher stone-free rate after mPCNL than after RIRS (OR: 2.12; 95% CI: 0.95-4.72; p=0.07) (Fig. 5).
5. Network Meta-Analysis of mPCNL, PCNL, and RIRS with Respect to Stone-free Rate
Network meta-analyses showed stone-free rates were similar after PCNL or mPCNL (OR: 0.96; 95% CI: 0.51-1.9). The stone-free rate after RIRS was lower than after mPCNL or PCNL (OR: 0.41; 95% CI: 0.21-0.82 and OR: 0.43; 95% CI: 0.22-0.82, respectively) (Fig. 8). The rank-probability test ranked mPCNL as No. 1 and RIRS as No. 3 (Fig. 10). The P-score test using the frequentist method to rank treatments in a network demonstrated that mPCNL (P-score: 0.820) was superior to PCNL (P-score: 0.680) and RIRS (P-score: 0) with respect to stone-free rate [48].
Funnel plots of retrograde intrarenal surgery (RIRS) and percutaneous nephrolithotomy (PCNL) (A), miniature percutaneous nephrolithotomy (mPCNL) and PCNL (B), and RIRS and mPCNL (C) success rates.
6. Network Meta-Analysis of mPCNL, PCNL, and RIRS with Respect to Length of Stay (LOS) and Operation Time
Thirteen studies had data regarding LOSs for two treatments. Five studies compared PCNL and mPCNL, seven studies compared PCNL and RIRS, and one study compared RIRS and mPCNL. In this network analysis, LOSs of patients treated by mPCNL (mean difference [MD]: -1.668; 95% CI: -2.311 to -1.320) or RIRS (MD: -1.281; 95% CI: -1.930 to -0.812) were shorter than for those treated by PCNL. No difference was detected between LOSs after mPCNL or RIRS (MD: -0.413; 95% CI: -1.188 to 0.386). The data of 21 studies were used to compare operation times. PCNL operation time was shorter than that of mPCNL (MD: -11.360; 95% CI: -14.290 to -7.455) and RIRS (MD: -7.224; 95% CI: -11.320 to -4.382), and operation time was shorter for RIRS than mPCNL (MD: -3.519; 95% CI: -5.442 to -2.175) (Table 2).
Subgroup network meta-analysis of lengths of stay and operation times (odds ratio and 95% credible interval)
7. Complication Rates according to the Clavien–Dindo Classification
Based on 23 studies, complication rates for mPCNL, PCNL, and RIRS were 19.0, 22.7, and 17.4, respectively. Major complication rates among all complication cases for PCNL, mPCNL, and RIRS were 7.4%, 12.5%, and 14.4%, respectively. However, no significant difference was found (p=0.13) (Table 3).

Complication rates of studies graded according to the Clavien–Dindo classification
DISCUSSION
Renal stones are one of the most common urological diseases and are characterized by high recurrence rates [49]. In cases of asymptomatic, tiny renal stones, observation can be performed without treatment. However, if a stone causes obstruction or infection, is associated with symptoms, such as pain or hematuria, or has a high probability of size increase, treatment is recommended. Interventional treatment for renal stones may be considered if a stone is greater than 1.5 cm or stone removal is necessary for social reasons. The EAU guideline recommends ESWL or RIRS as first-line treatments for kidney stones <2 cm in diameter and PCNL as the first-line treatment for stones >2 cm [7]. As regards surgical procedures, PCNL and RIRS have associated anesthetic burdens, and their invasivenesses are a disadvantage, but stone-free rates of PCNL and RIRS are higher than those of ESWL [50]. The development of surgical techniques and instruments continues to play a major role in the popularization of PCNL and RIRS [49,51]. mPCNL is defined as PCNL performed using Amplantz sheaths of diameter 14-20 Fr [3,52] and has the advantage of reducing complications that may arise due to the use of larger instruments and sheaths [4].
Evaluations of perioperative and postoperative outcomes after surgical treatment of renal stones are essential. Stone-free rates, operative times, and complications may be appropriate indicators of perioperative and postoperative outcomes. Among these indicators, stone-free rate may be one of the most important outcomes in terms of avoiding the need for auxiliary treatment and complications related to residual fragments. Stone-free rate is correlated with stone burden, but notably, differences have been reported between procedures [53]. Furthermore, stone-free rate is the best indicator of the efficacy of different approaches [54]. According to previous reports, PCNL and mPCNL have higher stone-free rates than RIRS, although various imaging modalities were used.
In 2017, Kang et al. [55] conducted a systematic review and meta-analysis, in which updated evidence of stone-free rates after RIRS and PCNL for >2-cm renal stones were compared with a previous report. In their meta-analysis of stone-free rates, a forest plot produced using the random-effects model showed a risk ratio of 1.11 (95% CI: 1.02-1.21; p=0.01) in favor of PCNL. In 2014, Zheng et al. [56], in a meta-analysis, reported no difference between RIRS and PCNL in terms of stone-free rates for >2-cm renal stones. Kang et al. [55] conducted a meta-analysis on the study by Zheng et al. [56] and three additional articles, and all three additional studies reported lower stone-free rates after RIRS than after PCNL. Zhang et al. [57] examined the efficacy and safety of RIRS, PCNL, and SWL for the management of lower pole renal stones and concluded that PCNL is associated with the highest stone-free rate but at the expense of hospital stay. In 2015, Zhu et al. [58] performed meta-analysis on stone-free rates after mPCNL and PCNL and concluded that mPCNL is safe and effective with a stone-free rate comparable to that of PCNL. In addition, they found that mPCNL resulted in less bleeding, fewer transfusions, less pain, and shorter hospitalization. Another recent systematic review demonstrated that the smaller tracts used during mPCNL tend to be associated with significantly lower blood loss and the need for blood transfusion, but at the cost of a significantly longer procedure than standard PCNL [59]. The results of our study support these previous findings. Network meta-analysis showed that in terms of LOS, mPCNL and RIRS were superior to PCNL. However, regarding stone-free rates, mPCNL and PCNL were superior to RIRS, and no difference was found between mPCNL and PCNL (OR: 0.95; 95% CI: 0.51-1.9).
mPCNL is likely to be developed further because of the popularization of dilating instruments and the recently released miniature nephroscope and irrigation system. In 1998, Jackman et al. [60] used a 6.9-Fr rigid ureteroscope, a 7.2-Flexible ureteroscope, and a 7.7-Fr rigid offset pediatric cystoscope. MIP-M by Nagele et al. [51] (Karl Storz GmbH & Co. KG, Tuttlingen, Germany) and Miniperc by Lahme et al. [6] (Richard Wolff, Knittlingen, Germany) are miniature nephroscopic instruments with a typical single-step dilating system. In addition, mPCNL often provides even higher stone-free rates than conventional PCNL, perhaps because of the vacuum-cleaner effect [61].
The American Urological Association and the EAU have not presented specific recommendations for the use of mPCNL to treat renal stones. However, previously reported evidence shows that mPCNL can achieve outcomes similar to that of standard PCNL for renal stones >2 cm [24]. RIRS requires insertion of a flexible ureteroscope through a natural orifice and maybe a competitor of mPCNL for the treatment of renal stones, but not Staghorn stones [59]. However, it is clear the stone-free rate of mPCNL is superior to that of RIRS and that stones can be removed easily by mPCNL due to its vacuum-cleaner effect. On the other hand, the longer operation time of mPCNL may be a major disadvantage. In our network meta-analysis, the operation time of mPCNL was greater than those of PCNL and RIRS, and although no significant difference was observed between the complication rates of the three modalities, the total number of complications after PCNL was higher than after mPCNL and RIRS. A well-designed, prospective study is needed to provide a better understanding of the use of mPCNL and to explore its potential to replace PCNL.
CONCLUSIONS
Summarizing, PCNL and mPCNL had the highest stone-free rates for the surgical treatment of renal stones, and RIRS had the lowest stone-free rate and the lowest rank by the rank-probability test. Patient selection should be performed based on case complexity, and a well-designed prospective study is needed to improve understanding of the use of mPCNL.
SUPPLEMENTARY MATERIALS
Supplementary data can be found via https://doi.org/10.14777/uti.2022.17.1.14.
ACKNOWLEDGMENTS
This work was supported by Inha University Research Grant. All relevant data are provided within the manuscript and its Supporting Information files.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
AUTHORS CONTRIBUTIONS
D.H.K. participated in literature search, data aquisition, data analysis, statstical analysis and manuscript preparation. K.S.C. participated in manuscript review. D.Y.C. and D.K.K. participated in statstical analysis and manuscript editing. W.S.J. and H.D.J. participated in literature search, data aquisition and manuscript editing. J.Y.L. participated in study concept, design, literature search, data aquisition, data analysis, statstical analysis and manuscript review. All authors read and approved the final manuscript.